
Recommended
Recommended
More Related Content
Similar to 1Proposal Effectiveness of non-pharmacological in Compari.docx
Similar to 1Proposal Effectiveness of non-pharmacological in Compari.docx (20)
More from durantheseldine
More from durantheseldine (20)
Recently uploaded
Recently uploaded (20)
1Proposal Effectiveness of non-pharmacological in Compari.docx
- 1. 1 Proposal: Effectiveness of non-pharmacological in Comparison to Methylphenidate Stimulant Therapy Barbara Maclure 9/18/2022 2 Effectiveness of non-pharmacological in Comparison to Methylphenidate Stimulant Therapy Introduction Attentive–deficit hyperactivity is a psychological disorder that is well known, affecting both children and adults. Some of the associated symptoms that are associated with ADHD include inattention, hyperactivity, impulsivity, and difficulty in focusing. It is reported that in the United States, about 8.5% of children are affected by ADHD. In the treatment process, several ways have
- 2. been put into place. Despite the treatment, many studies reported that some treatment methods have side effects. Therefore, knowing the method that least has the side effects is crucial. This research proposal will play an essential role as it will identify whether non-pharmacological intervention, behavioral therapy, and stimulant therapy have the same results in children aged 4 to 8. Background of the study Dr. George first identified ADHD when he was a pediatrician. He noted that his patients had uncontrollable impulsive behavior. There was an introduction of the drug Benzedrine, which was approved as it showed to improve ADHD symptoms in children. In 1950 there was the introduction of Ritalin drugs which were used in ADHD treatment in both children and adolescents. (Holland & Higuera (2017). The drug that is used in the treatment of ADHD to date is Ritalin. Despite the doctors treating patients with ADHD symptoms from the 1930s, there was no actual definition of ADHD. Still, it was given much
- 3. attention in 1987 when the American Psychiatric Association (APA) redefinition of the disorder. 3 By 2020, approximately 7.1 million young children aging between 2-17 years with ADHD had been diagnosed. (Garbe (2018). Despite the prevalence of the disorder among children and adolescents, ADHD is also present in adulthood. In most cases, this disorder is noted when the child gets into the class and starts issues of failing to focus on the classroom. There are different forms of ADHD which entails hyperactive/impulsive type, inattentive type, or a combination of the two. There is a criterion that is customarily utilized in the treatment of ADHD. The parents and the teacher are required to document the children's symptoms for a period of six months. Research shows that ADHD is more common in males than women. One of the interventions utilized is stimulant therapy, considered standard treatment for children after reaching an appropriate age. The stimulus, for example, the medication, is said to have side
- 4. effects which can be either mild or severe. Some noticeable side effects include upset stomach, appetite change, heart abnormalities, tics, and weight loss. Although the treated symbols are 70-80% treated, there can be the utilization of other alternative therapies that do not require the use of stimulant medication and play an essential role in minimizing ADHD symptoms. The current research shows that approximately 9% of young children residing in United States are affected by ADHD. Using stimulant therapy is the primary treatment method for the symptoms. The current research also show that pharmacological therapy is an effective method of treatment of the symptoms. Between 2013 and 2019, there were over 5873 articles written about ADHD. The term “young children " was added to minimize the research and behavioral therapy benefits and stimulants' side effects. In addition to this expression, the number of articles was reduced to 500 and 200, while about fifty articles were related to the behavioral therapy treatment of children.
- 5. 4 To identify the gap in the research conducted to date, we shall look at the importance of behavioral therapy and Methylphenidate treatment. Use of behavioral Therapy Before the stimulant therapy initiative in children with ADHD, there was a recommendation for using behavioral therapy, an idea embraced in American Academy of Pediatrics (AAP). The main aim of behavioral therapy was to help the kids gain self-control, self- instruction, problem-solving ability, and modeling. Children with that ADHD has been diagnosed said to have a high likelihood of developing emotional problems in their life. Behavioral therapy can help children in their initial stages cope with the symptoms not only in childhood but also in their adult life. A study by Thyagarajan shows that involving the parent and provider in behavioral therapy in school-based children is crucial. This becomes important for the parent to be taught the behavioral therapy technique.
- 6. The study that CDC did in 2018 indicated that less than 50 %of the children practicing the stimulant therapy had initially practiced the behavioral therapy. Of the children aged between 4-5 years, only one out of five was taking the medication to treat ADHD instead of recommending the use of behavioral therapy. This study also identified variations in the use of behavioral treatment from State to State. (Thyagarajan (2019) The study showed that all those states that opted to utilize behavioral therapy as the first line of treatment had decreased the number of children on the stimulate therapies. Most studies have put a lot of emphasis on combining behavioral therapy and stimulant medication. A study done in 2019 in 170 elementary schools indicated that combining both therapies improved results. Methylphenidate Treatment 5 This is the therapy that is most prescribed for children having ADHD. Several articles show
- 7. the adverse effects that are associated with the use of this therapy. One of the side effects that the study indicates concerning this therapy is Insomnia. One study found a change in the sleep pattern for the children who have undergone this treatment, especially when the therapy is done over a prolonged period. In 2019 a study was conducted on seventy- one children who had gone the treatment for six months. There was an indication that about 87% had a side effect. Some of the recorded side effects included irritability, Insomnia, and anorexia. Most studies showed that despite Methylphenidate being embraced, it had many side effects. Gap in Literature In most of the research that was done regarding Methylphenidate and behavioral therapies in children, no information concerning pre-school children and prevalence of the treatment in this age group. The research tends to show the presence of the symptoms that arise when a person experiences school life. An article published by the childhood & development Disorder identified several gaps. There is a gender gap when studying ADHD as the
- 8. studies gravitate toward males in the population. In availability of the voice of the children diagnosed with ADHD is also a big gap. It is worth noting that children cannot make medical decisions; thus, their voices are not heard based on their opinion. Listening to what they may feel after therapy could play a significant role in treatment. After the therapy, few studies follow up with the children to see the lifelong impact. Research Question and Hypothesis Research Question Lori Daniels First write in form of question (either a correlation or difference RQ) Lori Daniels same here. While you may find multiple gaps only the one(s) your RQ tests are relevant in this section Lori Daniels Ok, but will your study include children's opinions (which is qualitative?) Lori Daniels I'm not sure what you mean here Lori Daniels Only include gaps that lead to your RQ. If you were testing
- 9. gender in the RQ then you could mention a gender gap Lori Daniels remember prevalence by itself is not a testable RQ Lori Daniels Include a statement that reflects what is known and what isn't (so that it leads to your RQ). 6 The research to be conducted is to answer whether non- pharmacological therapy is the best alternative in treating attentive deficit hyperactivity disorder compared to using Methylphenidate stimulant therapy in children between 4-8 years. Hypothesis: Research and Null Using Behavioral therapy in treating school children between 4- 8 years is as effective as Methylphenidate stimulant therapy, evidenced by the behaviors of the teachers and the parents grading the study participant. Null Hypothesis: No difference exists between behavioral therapy and Methylphenidate interventions in the school children aged between 4 and 6 years. Nature of the study
- 10. In this study, the dependent variables in the behaviors will be keenly observed in the group participant on each treatment type. The qualitative independent variables present in the research are non-pharmacological treatment and Methylphenidate. The variable of operationalized will become the behavioral assessment to be completed by the teachers and parents regarding each participant's progress. Teachers and parents are required to grade the critical factors while determining the effectiveness of the independent variables. The nature of the study is qualitative experimental based. It will involve random selection of the participants so that the researcher will have maximum control. In the experimental study, only two variables are used to show their relationship. There is an experimental group and a control group. In this regard, the experiment group is children treated with behavioral therapy, while on the other hand, the controlled group is children undertaking Methylphenidate. The experiment group that is exposed to independent variables is behavioral therapy. The research will
- 11. Lori Daniels quantitative Lori Daniels what is the assessment (does it have a name?) Lori Daniels not qualitative just IV is fine Lori Daniels Missing what the difference is in (DV) Lori Daniels This should be in RQ as well (RQ and hypothesis include same words with RQ as a question) Lori Daniels avoid words like "best" because they are subjective. What will you use as a DV? That should be in RQ 7 be able have a comparison on the effects behavioral therapy symptoms of ADHD and the impact of behavioral treatment compared to Methylphenidate therapy. Study significance The paramount significance of this study is identifying whether non-pharmacological behavioral therapy is of the same effects on ADHD symptoms compared with stimulant therapy,
- 12. Methylphenidate. Implementing non-pharmacological interventions such as behavior therapy in the first line of medication in preschool and school-aged children can play an essential role in reducing stimulant use. Suppose the symptoms can be managed using non-pharmacological therapy such as behavioral therapy. In that case, the children cannot be at risk of the side effects associated with the use of the drugs. Many side effects result from the use of stimulant therapy. Some of these side effects are long run. It has come to my attention that most of the therapy have a short-term follow- up after the therapy. This research will not only help identify some of the short-term side effects of the use of the therapy on ADHD symptoms but also track the individual's progress. Some side effects which are said to be a result of the stimulant therapy will be looked at and dealt with amicably. This study is also essential since it will allow adolescents to speak their minds regarding the different therapies. Since the technology keeps improving, this study will look at the cheapest and most economical treatment.
- 13. Lori Daniels here is your DV. Make sure to include it in your RQ and hypothesis 8 References Attention-deficit/hyperactivity disorder (ADHD). (2018). Baum, Newman, Weinman, McManus, & West, (Eds.). (2018). Cambridge Handbook of Psychology, Health, and Medicine. Behavioral Therapy: Definition, Types, and effectiveness. (2016, November 14). CDC: AAP guidelines on behavioral therapy and ADHD in young children are not followed by most patients. (2015). Brown University Child & Adolescent Psychopharmacology Charach & Fernandez (2013, May 28). Enhancing ADHD Medication Adherence: Challenges and Opportunities. Current Psychiatry Reports, 15, 371. Helseth, Washbush, Gnagy, Onyango, Burrow-MacLean, Fabiano, Nicols-Lopez, K. (2015, April). Effects of behavioral and pharmacological therapies on peer reinforcement of deviancy in
- 14. children with ADHD-only, ADHD and conduct problems, and controls. Holland & Higuera (2017). The history of ADHD: A timeline. Khajehpiri, Mahmoudi-Gharaei, Faghihi, Karimzadeh, Khalili, & Mohammadi (2014). Adverse reactions of Methylphenidate in children with attention deficit hyperactivity disorder: Report from a referral center. Journal of research in pharmacy practice, 3(4), 130-6. Kholi, R(n.d.). The Early Childhood Attention Deficit Disorders Evaluation Scale (ECADDES) [Scholarly project]. Kraut, Langner, Lindemann, Banaschewski, Petermann, Petermann, Garbe (2018). Comorbidities in ADHD children treated with Methylphenidate: a database study. BMC Psychiatry, 13. Lynch, A. (2016, August 19). Identifying Knowledge Gaps in ADHD Research. Journal of Childhood & Developmental Disorders, McCarney, S. (1995). Early childhood attention deficit disorders evaluation scale (ECADDES). Lori Daniels
- 15. author initials are used in reference lists Lori Daniels italicize journal names Lori Daniels Use sentence case (mostly lower case) for article titles Lori Daniels incomplete reference 9 Palinkas, Horwitz, Green, Wisdom, Duan & Hoagwood (2015, September). Purposeful sampling for qualitative data collection and analysis in mixed method implementation research. Thyagarajan (2019). A case study using cognitive-behavioral therapy-management of ADHD. Indian Journal of Health & Wellbeing, 7, 471-477. Vigliano, Galloni, Bagnasco, Delia, Moledo, Mana & Cortese (2016, May). Sleep in children with attention-deficit/hyperactivity disorder (ADHD) before and after 6-month treatment with Methylphenidate: a pilot study. European Journal of Pediatrics, 175.
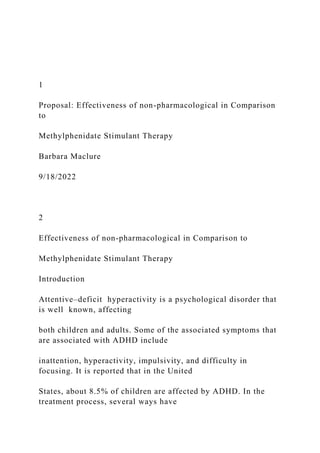
- 16. Comparison between Group A and B Numerical scale Average score The bar graph indicates that the behavioral therapy group had a higher average score on the ADHD Evaluation Scale than the Methylphenidate group, indicating that behavioral therapy is more effective in treating symptoms of ADHD. This supports the hypothesis that behavioral treatment is appropriate for ADHD compared to Methylphenidate stimulant therapy. Comparison Between Group A & B GROUP A (Methylphenidate therapy) GROUP B (Behavioral Therapy ) 3.56 1 1 Comparison of Therapies for children Diagnosed with ADHD
- 17. Barbara Maclure 10/03/22 2 Comparison of Therapies for children Diagnosed with ADHD Participants This study's participants will consist of 100 children (N=100) aged 4 to 6 years. This study will be conducted in the school where the children attend the class. The main reason behind selecting the school setting is because, in this setting, all the factors that affect work ethic, social interaction, and behavior will be considered. To conduct this study successfully, a class will be required to have 20- 25 students, their teacher, and our professionals. All the participants will be kindergarten children with who ADHD has been diagnosed. We will ensure that the sample size is large enough so that we will be able to collect data that will support or dispute the research question. Using one hundred participants surpasses the threshold; therefore, the data to be collected will have a weight to
- 18. support or dispute the research question. We will use purposeful sampling criteria to find one hundred students in the grade kindergarten aged 4-6 years. In qualitative research, it is essential to use purposeful sampling to get valuable data despite the limited resources. The children's choice will be based on pediatrician evaluations and diagnosis of ADHD. To get the participant, it will be ensured that they have not gone a treatment therapy before the start of the study. This is to facilitate the participant to be chosen randomly between methylphenidate treatment and behavioral therapy. The study will ensure that the parent consent of the children is taken. The participant will involve males and females. Measures In this study, the best research design is using qualitative experimental research. The main feature of experimental design is selecting the participant randomly; therefore, the research has a maximum control level. In much research for identifying a relationship between two or more Lori Daniels
- 19. quant Lori Daniels quantitative Lori Daniels I (you are the only author) Lori Daniels Methods (this is a continuation of Part 1) so place in one document 3 variables, they embrace experimental research. This research amicably compares two or more groups. Experimental research consists of both of experimental group and the control group. This experimental group will consist of the children undergoing medication or behavioral therapy; on the other hand, a control group entails children undergoing Methylphenidate. The experimental group gives an independent variable of behavioral therapy. The research will relate behavior therapy's effects symptoms of ADHD and the effect of Methylphenidate therapy on the same symptoms. Extraneous Variables
- 20. Many variables must be examined and recorded in observing and recording various issues related to ADHD children. No factors present in the children's classroom that may not have an indirect influence on the children's behaviors yet are not related to the ADHD symptoms. The presence of distractibility and peer influence are some of the core aspects that are likely to influence children's behaviors. The children can also be affected by the underlying situation related to ADHD and the comorbidities resulting from ADHD. Some of these variables cannot be fully monitored but can be closely checked concerning the study. Instrument The instrument used in this study to determine whether behavioral therapy is effective in Comparison to Methylphenidate therapy in treatment of ADHD is a numerical rating scale. Specifically, the study's scale will be the Children's Attentions deficit Evaluation scale. This scale was developed by different researchers that used the current literature in neurology, psychology, and education in modern practices of identifying other
- 21. individuals' diagnoses. (Buyx, 2019). The reliability of this scale is much dependent on the participant's faithfulness, but the validity of scale studies is so promising. 4 Using this scale in the schools and homes version plays an essential role in documentation of ADHD features in schools and home settings of children aged 2- 6 years. In most instances, the ADHD scales is constructed for children’s symptoms who are older; thus, this scale will be used as it evaluates the targeted age of the study. To some extent, this scale will be unique as it will enable both parents and teachers to participate in the ADHD symptoms present in the numerical scale. This scale will be part of the pre-diagnosis for ADHD and the accomplishing the research of the parents and teachers with a repetition of a questionnaire. This will enable the comparisons of the child questionnaire before behavioral and Methylphenidate therapy and provide answers if a reduction of symptoms is noted concerning the administered
- 22. treatment. Intervention Description Based on CDC, behavioral therapy is the first line of treatment for children under six years and having been diagnosed with ADHD is behavioral therapy. Behavioral medicine is essential in monitoring any negative behaviors resulting from ADHD. The principle used by behavioral therapy is that the behaviors are usually learned, and destructive behaviors can be modified. Psychologists can assist parents and children in focusing on the negative behaviors that arise from ADHD and the role to play in changing those behaviors. Some forms of behavioral therapy entail cognitive behavioral, aversion therapy, cognitive behavioral, and system desensitization. When working with both the children and the parents, the therapist can use on-form therapy or combine multiple of them based on their effectiveness Data Collection Procedure This study's participants will be based on the recommendation of pediatricians. The participant will involve children aged 4 to 6 years diagnosed with ADHD who
- 23. have yet to start the treatment. Before the participant's placement, it will be ensured that the parent's consent is obtained. Once the Lori Daniels Procedure (follow template for headings) 5 recommendation is made, and the parent signs the consent, the research will go to IRB to seek approval. The researcher will search the group using random means. Once the IRB verifies the approval, the participant will be grouped into two. Group A acts as control group, and group B acts as treatment group. 1. Group A a. There will be the prescription of the methylphenidate dosage of the participant by the Physicians b. The participant will be required to take Methylphenidate dosage every morning at 7 am before school. They will be taking the dosage at the same time c. It will be ensured that all the participants do not miss the
- 24. dosage of medication d. All side effects of Methylphenidate will be closely monitored 2. Group B a. In two months, the participant and parents will undergo eight behavioral therapy sessions with a well-trained psychologist. b. The teachers and parents will provide the positive behaviors identified c. The teachers and the parents will be required to have similar behavioral systems in the classroom and at home to have a consistency of participants. d. It will ensure that the participant has a consistent discipline band adequate structure. Data Analysis The research will be conducted in different demographics to have diverse participant groups. Male and females will be included in the study aged 4-6 years. The study will ensure that the participants are from different ethnic groups having the fulfillment of being diagnosed with 6
- 25. ADHD yet not started the treatment. Descriptive studies will be implemented to analyze the demographic, as shown IN the table below. Race Age Gender Grade Central Tendency Mean median Mode Standard Deviation Distribution Variance Dispersion In the analysis, ADHD symptoms score will be determined by ACADDES educators and parent questionnaires. The questionnaire will use a scale that ranges from 0 to 4. Zero indicates no sign of ADHD, and four exhibits ADHD behavior. The trial participants in the two available groups' scores will be done before that treatment when completion of the trial process is done.
- 26. The analysis is supposed to run through ECADDES computer system that will convert scores from raw to standards and percentiles, thus making the score to be more efficient. The descriptive statistics will consist of standard deviation, Variance and inference methods will be a t-test used to analyze data collected from the questionnaire. Comparison will be made in both groups to examine whether experimental group participants in the behavior therapy outcomes differed from the stimulant Methylphenidate control group. Lori Daniels You can remove this 7 Results The study is aimed at investigating the effectiveness of the treatment symptoms of ADHD between behavioral and Methylphenidate therapy. This research was guided by the hypothesis that stated non-pharmacology therapy is an appropriate therapy for ADHD compared to Methylphenidate stimulant therapy for children aged 4-6 years.
- 27. Based on the literature review, we can predict the real expectation of the results. For example, the CDC's study in 2018 indicated that less than 50 % of the children practicing stimulant therapy had initially practiced behavioral therapy. Of the children aged between 4-5 years, only one out of five was taking the medication to treat ADHD instead of recommending the use of behavioral therapy. This study also identified variations in the use of behavioral treatment from State to State. (Thyagarajan (2019) The study showed that all those states that opted to utilize behavioral therapy as the first line of treatment had decreased the number of children on the stimulate therapies. Most studies have put a lot of emphasis on combining behavioral therapy and stimulant medication. The current research also shows that pharmacological therapy is an effective method of treatment of the symptoms. The figure below shows the expected results of the side effects of the different therapies.
- 28. 8 1 2 3 4 5 0 0.5 1 1.5 2 2.5 3 3.5 4 Group A Group B Comparison of the Two Groups Group A Group B This indicates that the method B score is higher than A, thus more effective in treating ADHD. Discussion Ethical Issues
- 29. In conducting any research, there are incidences of ethical issues to arise, especially when using minor children. When performing the study involving children, it is essential to identify what the targeted population will benefit from the research. The central issue that requires to be addressed is whether the investigation will bring harm to children. (Freitag & Buyx (2019). In this research, the participant in the control group will receive Methylphenidate therapy which cannot endanger the participant or put them at risk from the medication. The parents will be well informed of the side effect through consent, and if the side effects arise, the pediatrician will check the patient. Despite the research being conducted in a school setting, it will be ensured that confidentiality and privacy will remain intact. The researcher will not require to expose the information on the progress of the teachers who is part of the evaluation process. Limitation of the study Lori Daniels The X axis should be 2 groups (not continuous)
- 30. Clarify what Y axis is (label) 9 The environment in which the research is conducted may become prone to biased results. The classroom environment may be subject to high stimulation from the children. It may be a rise in distractions that may result in poor results during the evaluation process. In addition, the person collecting the data may affect the performance. The teacher may score the students differently basing the criteria used, while the parents see them differently. The teacher and the parents can skew the score since they know the initial performance. To provide a resolution to this, it is essential to ensure that the participants are taken to classrooms where they are not familiar with their teachers. 10 References Shellenberg, Stoops, Lile & Rush (2020). An update on the
- 31. clinical pharmacology of Methylphenidate: therapeutic efficacy, abuse potential, and future considerations. Expert Review of Clinical Pharmacology, 13(8), 827. Jayamaha, Perera, Herath & Rodrigo (2018). A cross-sectional survey of adherence, perceived efficacy, and side effects of Methylphenidate among children at a teaching hospital in Sri Lanka. Masi, Fantozzi, Villafranca, Tacchi, Ricci, Ruglioni & Cortese (2019). Effects of melatonin in children with attention-deficit/hyperactivity disorder with sleep disorders after methylphenidate treatment. Neuropsychiatric disease and treatment, 15, 663. Sierawska, Prehn-Kristensen, Moliadze, Krauel, Nowak, Freitag & Buyx (2019). Unmet needs in children with attention deficit hyperactivity disorder—can transcranial direct current stimulation fill the gap? Promises and ethical challenges. Frontiers in psychiatry, 10, 334. Ghasemi, Nori & Abdi Zarrin (2019). The effect of parent management training (PMT) on the
- 32. reduction of behavioral symptoms in children with attention deficit hyperactivity disorder (ADHD). Quarterly Journal of Child Mental Health, 6(2), 9. Bussalb, Congedo, Barthélemy, Ojeda, Acquaviva, E., Delorme & Mayaud (2019). Clinical and experimental factors were influencing the efficacy of neurofeedback in ADHD: a meta- analysis. Frontiers in psychiatry, 10, 35. Nutrition 300 – Diet Project Part 2 Part 2 of your Diet Project is a diet and health evaluation. The purpose of this assignment is to compare your dietary intake (based on Diet Project Part 1) with the Dietary Reference Intakes (DRIs) and other nutrition recommendations. This evaluation is also meant to get you to think about what your diet is doing for you and what changes you can make to your diet to help you meet your nutrient goals. For Part 2 of this project, we will be evaluating our macronutrient (carbohydrates, protein, and fat) consumption. Directions: Fill in the tables and answer the questions based on the data from your Cronometer reports. You will need to refer to both the Trends and Servings reports that you submitted for Diet Project Part 1. Type in a different color text. Note: The Trendsreport will show you your average intake for each nutrient, so you DO NOT have to calculate any averages!
- 33. Please answer the questions based on the information from your Cronometer reports! · If a question does not apply to your situation, make sure to say something about it, such as “I’m not an athlete, so this doesn’t apply to me.” That way, I know you looked at the question. Don’t just skip the question! · I will be grading Part 2 using your Cronometer reports submitted for Part 1. If I see a food on Part 2 that wasn’t recorded on Part 1, or if there is a food I saw from Part 1 that should be on Part 2, you will lose points. Answer the questions based on what you are learning in this course! · You are required to explain your answers in detail, using your reports and knowledge about nutrition to support your answer. · Unacceptable responses: “it's junk/fast/processed food”, “it’s full of nutrients, ”“it’s healthier”, “it's better”, “I think my diet is healthy”, “I don’t like my diet”, or “my diet is horrible.” These will NOT earn you credit if you don’t explain why. Macronutrient Distribution - refer to the “Trends” report 1. Please fill in the following chart with the grams consumed, grams required, and & percentage met for your macronutrients (Protein, Carbs, Fat) from the “Macronutrient Targets” section (1 point) a. Note: the first number on the bar is the grams you ate, the number after the slash ( /) is your DRI or recommended amount, and the percentage is how much of your DRI you met.
- 34. Nutrient My Intakes (g) My DRI (g) Percent of DRI met Protein Net Carbs Fat 2. The percent of DRI met tells you what percent of your macronutrient goal you met. How did you do for each macronutrient? (1 point) 3. Is this what you expected from your diet? Or are you surprised by these results? (1 point) 4. Why or why not? Please explain your answer in detail. (2 points). Things to consider: what foods provided the most protein, carbs, fat? Are these foods part of your usual diet? Do you try to avoid or include certain foods? Are you following
- 35. any particular diet pattern? Carbohydrates - refer to the “Servings” and “Trends” reports 1. Look at your Servingsreport. Scroll over to the Carbs column. You can highlight the column to make it easier to read. Then look through all the numbers and find the top 5 highest carb amounts and the food that it corresponds to. Classify the main type of carbohydrate in that food as complex, simple, or concentrated/added sugar. See below or your lecture for descriptions (10 points): a. Complex carbs: foods with starch or fiber; ex: breads, cereals, pasta, vegetables, etc… b. Simple carbs: foods with mono or disaccharides; ex: fruits, 100% juice, plain milk/yogurt, etc… c. Added sugars: foods in which sugar has been added in processing or the sugar itself; ex: sugar, honey, cake, soda, sports drinks, cookies, candy, etc. NOTE: Some foods may contain more than one type of carbohydrate, you can identify it as more than one type where appropriate. Food item Carbohydrate provided (g) Complex, Simple, or Added Sugar 1.
- 36. 2. 3. 4. 5. 2. Based on the table in Question 1, do the majority of your carbohydrates come from Complex Carbohydrates, Simple Carbohydrates, or Added Simple Sugars? (1 point) 3. Based on Question 1, are over 50% of your carbohydrates from whole or refined sources (select one)? (Examples of whole sources: whole wheat, brown rice, oats, vegetables, fruit) (1 point) 4. What is a specific nutrient (do not just say vitamins and minerals, say which ones!) in whole sources and at least one health benefit of consuming whole sources over refined sources? (2 points)
- 37. 5. Looking at the Trends report under “ Carbohydrates”, fill in the following table (1 point) Type of carbohydrate Amount consumed (g) % of DRI met Fiber Starch No DRI Sugars No DRI 6. Out of the 3 carbohydrates in question 5, based on the amount you consumed in grams, which is the most predominant in your diet? (1 points) 7. How do you feel about the amount of fiber you are consuming? (1 point)
- 38. 8. The recommendations (DRI) for fiber are 25 grams for women and 38 grams for men. How many more grams of fiber would you need to eat in order to meet your Fiber DRI. Fill in the blanks below using the fiber amount from Question 5 and recommendations given. If you met the DRI, just write 0. (2 points) ________________ g - ____________ g = ____________________ g (your DRI for fiber minus the amount of fiber you consumed) 9. Look at your Fiber percentage in Question 5. If you did not eat the recommended amount of fiber (if you ate less than 75% of your DRI), select 6 foods that you could include in your diet to increase your fiber intake. You can use the diagrams on the next page to help or look up foods online. Include the food, the quantity you would eat, and the grams of fiber. If you met the DRI, write 0. (2 points) Food Quantity Dietary Fiber (g) 1. 2.
- 39. 3. 4. 5. 6. Proteins - refer to the “Trends” and “Servings” reports 1. Calculate your RDA for protein (2 points) Convert body weight in pounds to kg: _____________ pounds ÷ 2.2 pounds/kg = _____________ kg (your weight in pounds divided by 2.2 equals your weight in kg) _____________ kg body weight x 0.8g protein per kg bodyweight = _____________g/day (body weight in kg multiplied by 0.8 to give you your RDA for protein) If you are an athlete, you have an increased protein need. Please calculate your protein requirement using the range of grams/kilogram body weight below (from page 175 of your textbook). If you are not an athlete, you can skip this part and go straight to Question 2.
- 40. - For endurance athletes (long distance runners or cross- country skiers, triathletes) ______________kg body weight x 1.2 to 1.4g protein per kg bodyweight = _______ to _______g/day (body weight in kg multiplied by 1.2 & 1.4 to give you a range of protein that is your RDA for protein) - For strength athletes (weight lifters, body builders) _______________kg body weight x 1.2 to 1.7g protein per kg bodyweight = _______ to ______g/day (body weight in kg multiplied by 1.2 & 1.7 to give you a range of protein that is your RDA for protein) 2. According to the AMDR, protein should make up about 10- 35% of your total Calories. Let’s calculate your protein intake AMDR and see if you’re within your suggested range. (5 points) a. According to your Trends report under “ Energy Summary”, what was your average kcals consumed? = ________________ kcals/day b. Calculate the minimum protein recommendation below (10% of your average Calorie intake) _________________ kcals x 0.1 = ______________ kcals ÷ 4 = __________ g protein (average Calorie intake from 2a multiplied by 0.1, then divide by 4 kCal/g to get grams of protein) c. Calculate the maximum protein recommendation below (35%
- 41. of your average Calorie intake) _________________ kcals x 0.35 = ______________ kcals ÷ 4 = __________ g protein (average Calorie intake from 2a multiplied by 0.35, then divide by 4 kCal/g to get grams of protein) 3. According to your Trends report under the “ Protein” section, what was your average intake of protein? = __________ g (1 point) 4. Does your protein intake (from question 3) fall within the 10- 35% range calculated in Question 2b and 2c: (1 point): (bold or highlight one) Yes No Note: your protein AMDR range is calculated above with 2b being the low end and 2c being the high end. If your average intake falls into that range, you should highlight yes. If not, highlight no. 5. Looking at your “ Servings”report, find the top 10 HIGHEST sources of protein. If you have less than 10, that’s ok, just fill it out as much as you can. Then, classify the protein source as either complete or incomplete. (10 points) a. The easiest way to do this would be to scroll to the Protein column and highlight it. Then, go down the row and look at the food items that have the highest protein content. b. Even if a food has a little protein, if it’s the top 10, you should include it. c. If you ate something multiple times, you can list it multiple times on multiple lines.
- 42. d. If you have a mixed dish with complete and incomplete protein ingredients, you can say “both” Food Protein (g) Complete or incomplete? 1. 2. 3. 4. 5. 6. 7. 8. 9. 10.
- 43. 6. What are the potential disadvantages to consuming high amounts of complete proteins? (1 point) 7. What are the potential disadvantages to consuming high amounts of incomplete proteins? (1 point) Fats - refer to the “Trends” and “Servings” reports 1. Using your Trends report, please fill out the following table: (1 point) My Intakes Total Kilocalories consumed (kcals) (from the “Energy Summary” section) Total Fat (g) (from the “Lipids” section, the first row is the Total Fat row) Saturated Fat (g) (from the “Lipids” section) 2. Determine the % of total Calories that you consumed from total fat and saturated fat. (Hint: use the numbers from the chart above to complete the following calculations) (2 points) [_______ g (
- 44. Fat, Total) ÷ kcal consumed] x 9kcal/g x 100 = ______________ % [Your intake of grams of total fat ÷ total kcal] x 9kcal/g x 100 = percent of Calories coming from Total fat [_______ g ( Saturated fat) ÷ kcal consumed] x 9kcal/g x 100 = ______________ % [Your intake of grams of saturated fat ÷ total kcal] x 9kcal/g x 100 = percent of Calories coming from Saturated fat 3. How do your fat intake percentages calculated above compare to current recommendations for total fat and saturated fat below? Are you within the range for total fat and saturated fat? (2 points) · Recommendation for total fat: 20-35% · Recommendation for saturated fat: <10% of total calories 4. Did you expect to be within the recommendations for fat and
- 45. saturated fat? Why/why not? Explain your answer in detail. (Ex: what did you expect? Why did you expect that? What do you know about those foods? Do you try to avoid certain foods? Eat a lot of certain foods known to have high amounts of fat, etc…) (2 points) 5. Using your Servings report, identify the top 5 foods that are highest in saturated fat. (2 points) Note: scroll to the Saturated Fat column and highlight it. Then, go down the rows and bold the 6 highest saturated fat amounts. Then, see what food that saturated fat content corresponds to. Food Saturated Fat (g) 1. 2. 3. 4. 5
- 46. 6. Are you worried about your saturated fat intake? Why or why not? Compare your intake to what you calculated in question 3. (2 points) 7. What types of health conditions can be related to high saturated fat consumption? (1 point) 8. Using your Trends report, fill out the following table about Omega 6 and Omega 3 fat intake. (1 point) DRI My Intakes (g) Omega-3 Women: 1.1 grams Men: 1.6 grams Omega-6 Women: 12 grams Men: 17 grams 9. Compare your intake to the DRIs in the table. Are you meeting your DRI for Omega-3 and 6? (2 points)
- 47. 10. Looking at your Servings report, what 3 foods provide the most Omega- 3? (2 points) Food Omega-3 1. 2. 3. 11. Using the table to the right or your textbook, what other foods could you realistically eat to add more Omega-3 to your diet? (1 point) 1 image4.png image1.jpeg image2.png image3.png