Call Girls Darjeeling Just Call 9907093804 Top Class Call Girl Service Available
Iritis
1. Iritis (uveitis)
Presentation
The patient usually complains of unilateral eye pain, blurred vision and photophobia. He
may have had a pink eye for a few days, trauma during the previous day, or no overt
eye problems. There may be tearing but there is ususally no discharge. Eye pain is not
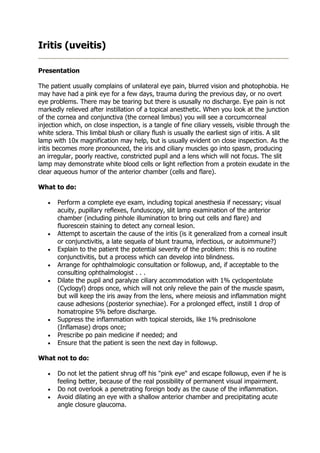
markedly relieved after instillation of a topical anesthetic. When you look at the junction
of the cornea and conjunctiva (the corneal limbus) you will see a corcumcorneal
injection which, on close inspection, is a tangle of fine ciliary vessels, visible through the
white sclera. This limbal blush or ciliary flush is usually the earliest sign of iritis. A slit
lamp with 10x magnification may help, but is usually evident on close inspection. As the
iritis becomes more pronounced, the iris and ciliary muscles go into spasm, producing
an irregular, poorly reactive, constricted pupil and a lens which will not focus. The slit
lamp may demonstrate white blood cells or light reflection from a protein exudate in the
clear aqueous humor of the anterior chamber (cells and flare).
What to do:
• Perform a complete eye exam, including topical anesthesia if necessary; visual
acuity, pupillary reflexes, funduscopy, slit lamp examination of the anterior
chamber (including pinhole illumination to bring out cells and flare) and
fluorescein staining to detect any corneal lesion.
• Attempt to ascertain the cause of the iritis (is it generalized from a corneal insult
or conjunctivitis, a late sequela of blunt trauma, infectious, or autoimmune?)
• Explain to the patient the potential severity of the problem: this is no routine
conjunctivitis, but a process which can develop into blindness.
• Arrange for ophthalmologic consultation or followup, and, if acceptable to the
consulting ophthalmologist . . .
• Dilate the pupil and paralyze ciliary accommodation with 1% cyclopentolate
(Cyclogyl) drops once, which will not only relieve the pain of the muscle spasm,
but will keep the iris away from the lens, where meiosis and inflammation might
cause adhesions (posterior synechiae). For a prolonged effect, instill 1 drop of
homatropine 5% before discharge.
• Suppress the inflammation with topical steroids, like 1% prednisolone
(Inflamase) drops once;
• Prescribe po pain medicine if needed; and
• Ensure that the patient is seen the next day in followup.
What not to do:
• Do not let the patient shrug off his "pink eye" and escape followup, even if he is
feeling better, because of the real possibility of permanent visual impairment.
• Do not overlook a penetrating foreign body as the cause of the inflammation.
• Avoid dilating an eye with a shallow anterior chamber and precipitating acute
angle closure glaucoma.
2. Discussion
Iritis (or anterior uveitis) always represents a real threat to vision which requires
emergency treatment and expert followup. The inflammatory process in the anterior
eye can opacify the anterior chamber, deform the iris or lens, scar them together, or
extend into adjacent structures. Posterior synechiae can potentiate cataracts and
glaucoma. Treatment with topical steroids can backfire if the process is caused by an
infection (especially herpes keratitis); thus the slit lamp examination is especially useful.
Iritis may have no apparent cause, or be associated with ankylosing spondylitis, Reiter's
syndroms, psoriatic arthritis, sarcoidosis and infections such as tuberculosis, Lyme
disease and syphilis.
Sometimes an intense conjunctivitis or keratitis may produce some sympathetic limbal
blush, which will resolve as the primary process resolves, and require no additional
treatment. A more definite, but still mild, iritis, may resolve with cycloplegics, and not
require steroids. All of these, however, mandate ophthalmologic consultation and
followup.