
Recommended
More Related Content
Similar to Chapter 29 Simulation in Healthcare EducationValerie HowardKim.docx
Similar to Chapter 29 Simulation in Healthcare EducationValerie HowardKim.docx (20)
More from cravennichole326
More from cravennichole326 (20)
Recently uploaded
Recently uploaded (20)
Chapter 29 Simulation in Healthcare EducationValerie HowardKim.docx
- 1. Chapter 29 Simulation in Healthcare Education Valerie Howard Kim Leighton Teresa Gore The emergence of technology for educational purposes creates a need for faculty and health science educators to understand how to not only operate the technology but also implement it within the academic and service settings while still using sound academic principles. Objectives At the completion of this chapter the reader will be prepared to: 1.Define the different types of simulation modalities available 2.Describe the challenges and opportunities inherent to simulation 3.Apply the Standards of Best Practice: Simulation to the simulation lab 4.Discuss the use of simulation-based education in interprofessional experiences 5.Analyze the similarities and differences related to the available simulation resources 6.Develop evidence-based simulation activities for graduate- level education Key Terms Clinical scenario, 459 Debriefing, 461 Fidelity, 455 Learning environment, 457 Simulation, 454 Simulation experience, 457 Standards of Best Practice: Simulation, 460
- 2. Abstract The use of simulated learning experiences has rapidly emerged in healthcare education as a method of training healthcare providers in a safe environment without subjecting patients to harm. Multiple definitions of simulation-related terms exist, so the importance of the use of standardized terminology is stressed. Best practice standards for implementing simulated learning experiences are discussed in this chapter. These should be provided in a standardized manner while adhering to guidelines to maximize learning. Simulated learning experiences directly correlate with the Core Competencies for Interprofessional Collaborative Practice. Finally, issues, challenges, and opportunities for the future of healthcare education and the use of simulation are outlined. Introduction Simulation is a time-honored method of teaching that has been used in health education for decades. It is defined as the use of “one or more typologies to promote, improve, and/or validate a participant's progression from novice to expert,”1(pS6) where the novice to expert continuum is consistent with that promoted by Benner.2 Experiential learning theory is used in health professions education to emphasize the importance of clinical practice in the educational process.3 Simulation is one method of experiential, hands-on application learning and can range from a simple activity used to mimic reality (e.g., the process of injecting an orange to create the feel of puncturing skin) to the use of high-fidelity simulation to create the comprehensive experience of interacting with a healthcare team during a clinical emergency. In each case the simulated clinical experience “includes pre-briefing, the clinical scenario, and debriefing; it is the engagement part of a clinical scenario.”1(pS6) Types of Simulations Several types of simulation are used in healthcare education, including written case studies, computer models such as Second Life, standardized patients, partial task trainers, and medium- to
- 3. high-fidelity patient simulators. Simulators are used to help students to improve critical thinking, clinical judgment, communication, and teamwork skills while assisting learners to meet psychomotor, cognitive, and affective learning objectives. Most of the growth in simulation is with standardized patients, task trainers, and simulators. Standardized patients consistently portray a patient or other individual in a scripted scenario for the purposes of instruction, practice, or evaluation.4 Standardized patients may be actors who require little training. Others may be people who respond to requests for assistance with healthcare training and require significant resources for training. Still others may actually have the disease, illness, symptom, or injury under study. In most cases standardized patients are paid for their assistance to the educational process. Partial task trainers typically represent anatomic parts of the human body and are used to practice skill acquisition.5 This type of simulator assists learners to meet psychomotor objectives, those accomplished when a student demonstrates the ability to perform a task such as inserting a urinary catheter, giving an injection, or attaching a heart monitor. Partial task trainers can range from low to high levels of realism. Examples of low-realism partial task trainers are when learners practice giving intradermal injections using a silicone pad that is flexible enough to allow a bleb to form when fluid is injected or using a hot dog with skin for the same purpose. An example of a more realistic partial task trainer is a model that promotes practice of intravenous needle insertion through a virtual model that includes haptic technology. Haptics is a feature allowing tactile sensation, for example, when the needle enters a vein. Simulators include full-body mannequins and can range from static mannequins that do not respond to any intervention to high-fidelity computerized simulators designed to realistically respond to learner interventions. High-fidelity mannequins can have blinking eyes, a chest that rises and falls with breaths, heart and lung sounds, and palpable peripheral pulses and can
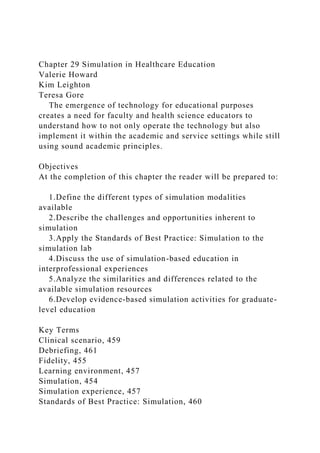
- 4. be capable of being intubated, having chest tubes inserted, and having other assessments and procedures performed on them. High-fidelity simulators are particularly useful for interprofessional training on cooperative activities such as codes. An example is the mannequin shown in Figure 29-1 marketed by Laerdal. These simulators are considered the most lifelike compared to human patients. The most realistic simulators in healthcare education are, of course, real persons. Obviously, numerous skills and conditions cannot be recreated for safety reasons. Instead, educators often use a hybrid simulation involving two types of simulators. A FIG 29-1 Sample high-fidelity simulator. (Photo courtesy of Laerdal Medical Corporation.) student can explain the procedure, risks, and potential complications to the standardized patient while performing the procedure on the partial task trainer. Standardized patients can assist learners to meet objectives while enhancing communication, clinical judgment, critical thinking, and teamwork skills. Fidelity Fidelity is the standard term used to describe the realism involved in simulated learning activities. There are a variety of ways to create fidelity in the learning experience, which can be confusing for educators. It recently has been recognized that fidelity has very little to do with what equipment is used and much more to do with how that equipment is used. Fidelity can involve a variety of dimensions, including the following: •Physical factors such as environment, equipment, and related tools •Psychological factors such as the emotions, beliefs, and self-awareness of participants •Social factors such as participant and instructor motivation and goals •Culture of the group
- 5. •Degree of openness and trust, as well as participants' modes of thinking1(pS5) On a trajectory from low fidelity to high fidelity, task trainers are considered of lower fidelity than high-fidelity simulators and finally standardized patients. However, this type of classification is not without controversy. Alinier places computer-controlled simulators above standardized patients in his continuum.6 For example, a high-fidelity mannequin used in a cardiopulmonary arrest situation may not even be turned on, depending on the level of the learner. A low-fidelity task trainer used in a high-fidelity environment may allow the combination to rank higher than the task trainer alone. Other types of simulation (e.g., written, screen-based) fall into the trajectory, depending on how they are used. The decision about the level of fidelity needed for any simulated clinical experience should always be based on the learning objectives. Thus it is not always necessary to have high fidelity, especially when cost as well as technology needs are both considered. The example in Table 29-1 involves inserting a central line. The most common fidelity consideration is the type of simulator to be used; however, educators have become aware of additional types of fidelity such as environment. Fidelity of the environment considers the location in which the simulated clinical experience takes place. A high-fidelity mannequin may need to be used within a psychomotor skills lab, a classroom, or even office space. An environment most similar to where real patient care takes place is highly desirable. Additionally, the equipment, furniture, and supplies should all be as realistic as possible to the traditional clinical environment. Creating methods to add patients' emotions, beliefs, spirituality, culture, and communication are also ways to make the experience more realistic. Table 29-2 outlines ideas for meeting learning needs in the developmental, spiritual, sociocultural, and psychological dimensions. Benefits of Simulation
- 6. Simulation offers the chance for learners to practice in a safe environment without placing patients at risk. Simulation significantly increases learners' knowledge,7,8 competence,9 self-efficacy,10 and confidence11 at no added risk to patients. While the former are intermediate outcomes, a longer-term outcome of better training is higher quality of patient care. Deliberate practice, the process of practicing a skill multiple times until mastery is reached, is facilitated within the simulation environment through the use of task trainers, further reducing the risk of harm to patients.9 Simulation also offers the opportunity to create standardized learning experiences in a controlled environment and provides exposure to low- occurrence, high-risk situations with opportunities to practice critical thinking skills, problem solving, and decision making. TABLE 29-1 Fidelity Correlated with Objectives OBJECTIVE: THE LEARNER WILL … TYPE OF SIMULATOR Accurately place central line catheter Task trainer Maintain sterile technique when placing a central line Task trainer Clearly communicate risks when obtaining consent from patient Standardized patient Use various communication techniques to calm patient's anxiety Standardized patient Recognize need for central line insertion during hypertensive crisis High-fidelity simulator Insert central line when rapid blood transfusion is required
- 7. High-fidelity simulator TABLE 29-2 Dimensions of Learning and Fidelity DIMENSION SIMULATED PATIENT IMPROVING FIDELITY Developmental 42-year-old male patient with myocardial infarction (MI); works as laborer Place frame with picture of young family at bedside. Does the learner recognize that patient likely will not be able to return to work? Does he or she consider how the family will have their financial needs met? Spiritual Patient will be having emergent surgery Place religious or spiritual book or icon at the bedside. Does the learner recognize the need to ask the patient about his or her beliefs and practices? Sociocultural Patient is being discharged with five new prescriptions Provide discharge instruction sheet. Does the learner determine whether the patient has the resources to get new prescriptions filled? Psychological Postoperative knee replacement patient cannot return home to care for self The patient reveals that there are 10 steps before entering his
- 8. home. Does the learner explore how the patient feels about the loss of his or her independence? An evaluation of any educational training program should align with evaluation models of training, for example, Kirkpatrick's model.12 Kirkpatrick identified the following four different levels of outcomes of training programs: •Level 1: Reaction, measures the learners' reactions to the training program. For example, were the learners satisfied with the program and how do they plan to use the information provided? •Level 2: Learning, measures the amount of knowledge, attitudes, or skills that have changed and the level of the change as a result of the training. •Level 3: Behavior or Training Transfer, measures the amount of “on the job” behavior change by the learner following the training sessions. •Level 4: Results, measures the organizational impact of the training program, on either performance or cost savings. Much of the research related to simulation has focused on the first two levels, measuring the learner's perspective, satisfaction, and knowledge gain related to the experience. However, ultimately simulation researchers will want to demonstrate the benefit of simulation training and its impact on patient outcomes (level 4). As an example, most recently simulation training has been correlated with lower central line infection rates,13 decreased complications resulting from shoulder dystocia obstetrical emergencies,14 and healthcare cost savings related to decreased malpractice claims.15 Challenges and Opportunities While simulation is an ideal environment for creating standardized learning opportunities and applying theoretical knowledge in the practice setting, inherent challenges exist related to the ease of implementation. Cost
- 9. High-fidelity simulation mannequins can be expensive to purchase and maintain. Highly computerized mannequins can cost between $30,000 and $125,000 while task trainers can cost as little as $250 depending on the level of complexity and fidelity. Standardized patient experiences also have higher costs because of the need to hire and train actors. Hourly pay for actors differs depending on the region and the level of the actors' experience but can range between $12 and $40 per hour. Educators need to factor in time for preparation, training, and participation per actor. If the simulation center is recording each simulation experience for use in debriefing, as is typical, the audiovisual software systems can cost between $10,000 and $50,000 per simulation room depending on the functions needed and levels of complexity. In addition to costs related to the simulation modalities, financial resources must be committed to support the center and faculty time and training. Resource considerations can include workload release time to learn and understand how to use the simulation technology and how to implement simulations into the curriculum, funding for conference attendance, purchase of related journals and books, and membership dues for simulation organizations. After the initial purchase costs, annual maintenance funds are required. These costs include ongoing maintenance, depreciation, and upgrades to the technology. Extended warranties can be purchased to cover the ongoing maintenance needed to ensure proper working order of the computerized mannequins. Most simulator mannequins are classified as capital purchases, so it is important to discuss the purchase, maintenance, and any insurance coverage with your institution's business office prior to making a commitment. Also, when planning for a simulation mannequin purchase, consider budgeting for costs related to replacement parts. Each piece of simulation equipment may have different suggestions related to replacement parts, including “skins,” appendages, and moulage, so it is important to have conversations with simulation vendors prior to purchase so that appropriate budgetary planning and
- 10. projections can begin. Many health professional programs include student simulation lab fees. Others may seek grant funding from foundations, corporations, or private donors to support these efforts. Funding success can be maximized by developing a relationship with the potential funder, correlating the funding proposal with the mission and vision of the funding agency, and forming collaborative partnerships to demonstrate a unique and sustainable project. Technology The high-fidelity simulation mannequins can be difficult to operate by faculty who lack technological experience or knowledge. In addition, skills are required to operate the digital audiovisual equipment to record simulation experiences. Box 29-1 Job Description for Simulation Technician Under the direction of the Simulation Center Director, the technician will provide technical support for all simulation experiences and operations, including preparation, maintenance and repair of computerized mannequins, task trainers, simulation-related hardware and software systems, audiovisual equipment, administrative website management, and digital recording systems. Partnering with simulation vendors may allow specific training opportunities to enhance understanding of the simulator technology and promote ease of use. Hiring a full-time or part- time simulation technician may be necessary. Generally, previous experience with computers, information technology, and even sound or recording can enhance the effectiveness of the simulation technology. Box 29-1 offers a sample job description for a simulation technician. Informatics principles and processes can be used for simulation projects and for developing simulation centers. For example, the systems life cycle (SLC) introduced in Chapter 2 can be applied to the purchase and installation of products. To review, the phases of the SLC are as follows:
- 11. 1.Analyze 2.Plan 3.Develop or purchase 4.Test 5.Implement or go-live 6.Maintain and evolve 7.Evaluate 8.Return to analyze The SLC is tailored to the project at hand; however, the processes and activities are similar to those used for any other project. Faculty Development Simulation is just one example of an experiential teaching and learning strategy, but many faculty lack the understanding of educational principles related to the best methods for implementing experiential learning strategies within the curriculum. Therefore knowledge of the following educational principles will assist the simulation facilitator in developing academically sound experiences: •Educational theory •Application of theory to practice •Development of clear and measurable objectives •Instructional design •Formative and summative learner evaluation •Program evaluation •Facilitation of learning •Debriefing strategies •Creating a safe learning environment in the simulation lab To maintain a safe environment for learning and ensure commitment to academic principles, each simulation facilitator should have an orientation period to learn the aforementioned principles and observe experienced simulation facilitators, similar to a mentorship model. If schools do not have the
- 12. appropriate experts within their organizations, resources should be committed to educate the simulation facilitator. Likewise, institutions will need to develop policies that require the simulation facilitator to have appropriate training before interacting with learners in the lab. Several organizations, such as the International Nursing Association for Clinical Simulation and Learning (INACSL), the National League for Nursing (NLN), the American Association of Colleges of Nursing (AACN), and the Society for Simulation in Healthcare (SSH), offer annual meetings, conferences, and faculty development webinars to assist with this challenge. In addition, several higher education institutions offer graduate-level certificates with concentrations in simulation. Two scholarly journals are devoted to simulation: Clinical Simulation in Nursing and Simulation in Healthcare. Finally, other organizations offer continuing education programs with continuing education credits for their ongoing developmental programs. TABLE 29-3 Kotter's Principles Applied to Simulation KOTTER'S PRINCIPLE APPLICATION TO SIMULATION EDUCATION Creating a sense of urgency • Identify the need for simulation based training within institution • Share simulation based research and evidence with stakeholders Developing a guiding coalition • Identify simulation champions and other like-minded individuals in your organization to form your simulation team • Choose representatives from all stakeholders (faculty,
- 13. administrators, clinicians, educators, learners, students, staff, patients, families) Developing a vision • Develop a mission, vision, name, and strategic plan for your simulation program or center • Create a business plan • Include input from all stakeholders Communicating that vision • Share the plan with all stakeholders • Use a marketing or branding approach for the name of your organization • Consult with your public relations department Empowering stakeholders to act upon that vision • Develop an organizational structure to support each team member • Schedule regular meetings for progress updates and document the minutes from each meeting • Develop clear and concise roles and responsibilities for simulation related activities and ensure accountability • Seek resources from administration, outside funding agencies, participant fees to support the structure Create short term wins • Develop one or two simulation activities based upon sound educational principles and implement this according to the best
- 14. simulation evidence available • Celebrate the successes of each individual in your simulation team Consolidation of improvements • Collect data on each simulation experience and use the data to improve quality Institutionalizing new approaches • Develop and implement policies and procedures related to simulation (i.e.: simulation facilitator, facilitation, simulation design, scheduling, debriefing) • Maximize use of your simulation center • Continue to share the positive simulation evaluation data, both quantitative and qualitative, with administrators, faculty, clinicians, educators, and all stakeholders Adapted from Kotter, JP. Leading Change. Boston, MA: Harvard Business Review Press; 1996. Faculty or Administrative Buy-In The use of simulation modalities to enhance learning can be considered an organizational change and resistance to change efforts has been widely reported in all disciplines, including business, organizational behavior, psychology, and healthcare. Faculty may be resistant to learning the new technology, administrators may not understand the importance of dedicating time and resources to the successful implementation of the simulation efforts, and students may be anxious about the possibility of being recorded as they practice in the simulation center. Successful change efforts can be facilitated by having a thorough understanding of change theories and using this
- 15. theoretical knowledge to guide the efforts. One change model used in healthcare was developed by John Kotter, who suggests following eight steps when leading a change effort (Table 29- 3).16 These steps can be applied to simulation efforts with health practitioners. Creating a mission and vision statement for the simulation program and developing a strategic plan can also guide future efforts related to integrating advanced practice experiences within the simulation program.17 Evaluating the participants' satisfaction related to the simulation experiences through the use of postsimulation surveys can also provide necessary data to share with administrators in an effort to gain support. Faculty members can be given an opportunity to visit the simulation lab and experience first-hand the learners' reaction to this powerful educational tool. Finally, sharing the positive experiences of students both quantitatively and qualitatively, through reflections and stories, can also generate buy-in. The Simulation Process Learning Theories Applied to Simulation Simulation is often accepted without any validation and based on the technology instead of a theoretical underpinning. Kneebone identified the following four areas for using theoretical underpinning: 1.Gaining technical proficiency with psychomotor skills 2.Learning theory with repetitive practice and frequent reinforcement 3.Tailoring support to the individual learner's need using situated learning 4.Addressing the affective domain of emotions with learning18 In addition, Kneebone identified the following four criteria for evaluating existing and new simulations: 1.Allow sustained, repetitive, and purposeful practice in a
- 16. safe, controlled environment 2.Level interaction with the expert or mentor depending on the proficiency of the student 3.Simulation should mimic actual life experiences 4.The simulated environment should foster a learner-centered approach that inspires and supports students18 Through deliberate practice students can develop a foundation for incorporating evidence-based practice (EBP) in bedside patient care. This should result in better patient outcomes from safe, quality nurses.19–22 A foundation for a theoretical background for simulation can be based on experiential learning. Several experiential learning theories have been applied to the use of simulation, as follows.23–25 •Knowles' adult learning theory. This theory originally stated that adults learn differently due to andragogy (theory of adult learning).26 Characteristics of adult learners are that they are self-directed, want to be involved in planning and evaluating their learning experience, use past experiences to build new learning, need to understand the reason for learning, want immediate application of knowledge to solve problems, and are more invested when the learning is associated with a new role. In 1984 Knowles changed his position to recognize that the assumptions about andragogy are situation specific and not unique to adults.27 In 2010 Clapper expanded on this assumption regarding what adult learners wanted educators to know. These learners want educators to create a safe learning environment that uses active and collaborative learning experiences, encourage reflection on current and past experiences, and focus more on the assessment of improvements made instead of pure evaluation. •Kolb's experiential learning. This refers to a person's ability to transfer knowledge from theory into practice, thereby leading to acquisition of knowledge.28 Waldner and Olson combined
- 17. Benner's first three stages of learning (novice, advanced beginner, and competent) and Kolb's framework using high- fidelity patient simulation in academia.29 •Situated cognition. Learning occurs as a social activity incorporating the mind, the body, the activity, and the tools in a context that is complex and interactive. This incorporates all domains of learning: psychomotor, cognitive, and affective.27 •Lasater's Interactive Model of Clinical Judgment Development. Four areas of clinical judgment are noticing, interpreting, responding, and reflecting.30,31 This model can be applied to simulation for noticing and assessing patient situations and conditions, interpreting the assessment findings, responding by developing a plan of care and interventions, and reflecting during the debriefing process. •Jeffries/NLN simulation framework. This is a conceptual framework developed for use in nursing education to design, implement, and evaluate simulation experiences.32 This model depicts the triadic relationship of students, faculty, and educational practices and their influence on the simulation design and desired outcomes. The five possible outcomes of simulations are increased knowledge, skill performance, learner satisfaction, critical thinking abilities, and self-confidence of the participants. •Gaba's 11 dimensions of simulation. These are as follows: 1.The purpose and aims of simulation activity 2.Unit of participation 3.Experience level of participants 4.Healthcare domain in which simulation is applied 5.Healthcare disciplines of participants 6.Type of knowledge, skills, attitudes, or behavior addressed in simulation 7.Age of patient being simulated 8.Applicable or required technology 9.Site of simulation participation 10.Extent of direct participation 11.Feedback method accompanying simulation33(pp13-16)
- 18. For students to envision themselves successfully assuming a new role, practicing that role in a realistic environment will assist with role identification, mental visualization for performing in the role, and bridging the gap from didactic to practice. Through participating and acting in a specific simulation case the participants can then generalize the information in order to apply it to new situations.23,34 Best practices are available for many aspects of simulation practice. A clinical scenario should be developed based on the specific learning objectives of the participants. During the planning and development of a scenario it is important to construct an experience that is appropriate to the participant's level of learning as well as the participant's objective. Since many simulation experts believe that the majority of learning occurs during the debriefing process, a planned debriefing strategy should guide the facilitator in the process. The last aspect is the identification and application of a theoretical framework to plan and guide a simulation to provide the theoretical underpinning for that simulation and simulation program.1,32,34–36 These aspects will be explored further in the next section. Summary of Standards of Best Practice: Simulation Standards of Best Practice: Simulation was developed by the INACSL board of directors at the request of its membership after an extensive needs analysis was conducted via member email and listserv. The purpose of the analysis was to determine the priority and ranking of the INACSL membership. Top priorities were established as standards and the lower priorities are under development as guidelines. The work of the Standards Committee is ongoing, with a current focus on developing guidelines to support the standards. Simulation standards have been developed to assist with the planning and implementation of simulation experiences.6 Following Standards of Best Practice: Simulation will likely lead to better learning experiences and improved learning outcomes for participants.
- 19. The first seven standards were presented at the 2011 conference and published for all members in the fall of 2011 by Elsevier. These initial standards are terminology, professional integrity of the participants, participant objectives, facilitation methods, simulation facilitator, the debriefing process, and evaluation of expected outcomes. Standards and Their Application to the Simulation Process The simulation experience will depend on the objectives to be obtained by the participants. The objectives are the guiding principle of the entire simulation. Once the objectives have been established, the level or type of facilitation should be determined based on the level of experience of the participants and the type of evaluation of the participants. The simulation process should follow the steps outlined in Box 29-2 in designing the scenario or experience to assist the participants in achieving the objectives. Standard I: Terminology The main terminology used in simulation is defined based on a review of literature. To begin the simulation experiences, have standard definitions for the application and possible publication and replication of research and evidence-based practices.37 Also, with more emphasis on interprofessional collaboration, standardized terminology is the key to increasing understanding between team members by not having only one discipline's terminology used. Box 29-2 Steps for the Simulation Process 1. Assign the presimulation or prescenario exercises to be completed by the participants 2. Prebriefing sessions immediately prior to the simulation 3. Simulation scenario with appropriate facilitation by a trained facilitator 4. Debriefing and/or guided reflection 5. Postsimulation exercises Standard II: Professional Integrity of the Participants
- 20. Prior to beginning any simulation the participants need to be oriented to the simulation program and understand the need for professional integrity to maintain confidentiality and integrity of the simulation.38 Professional integrity is needed in order for all participants to have the same learning experience. If participants share what occurred in the simulation with future participants prior to the simulation, then those participants do not have the same opportunity to use critical thinking and clinical judgment. This could affect their confidence level and take away learning experiences. Participants must be informed of the type of evaluation and expectations prior to any simulation. Standard III: Participant Objectives The simulated clinical experience should focus on course, clinical, or program objectives and be based on the participants' level of experience rather than on the fidelity of the equipment. The technology does not guide the learning but rather is a supplement to the educational experience. It is important to identify the methodology for implementing the scenario prior to the simulation to construct the best learning experience for participants. This will provide a foundation or guide for the simulation experience by identifying the appropriate scenario, the level of fidelity (mannequin, standardized patient, or a hybrid), the type of facilitating, the facilitator, and the environment.33,34,39 There is no evidence that suggests or dictates a specific time recommendation for each scenario. The scenario time should be based on the time required to meet the objectives; however, a time limit should be identified for each scenario. Some commercially purchased simulation products incorporate presimulation (prescenario) and postsimulation (postscenario) exercises for undergraduate education; however, this is not available for graduate-level education at this time. Presimulation or prescenario exercises are designed to prepare the student for participation in the simulation. Prescenario exercises are to be completed by the participants prior to
- 21. participating in the simulation and can include, but are not limited to, reading assignments for major concepts in the simulation, pretest questions, skills review, and audiovisual material. Standard IV: Facilitation Methods Facilitation type should be determined by the level of the participant and the type of evaluation.40,41 Several types of facilitation are instructor driven, partial instructor driven, or participant driven. As might be obvious from the labels, beginning participants usually require more instructor cueing or prompting (instructor driven). As the level of experience increases, less instructor prompting is required (partial instructor driven). During a summative evaluation, such as high-stakes testing, minimal to no prompting by the instructor is performed (participant driven). Standard V: Simulation Facilitator The facilitator is the major component that provides the link between the scenario and the participant to provide guidance for meeting the objectives of the simulation. The role of the facilitator is to adjust the scenario to respond to the actions or inactions of the participants according to the objectives of the scenario. The facilitator also leads the participants in the debriefing process in a positive manner to reflect on ways to improve the care provided for better patient outcomes.41 Standard VI: The Debriefing Process The purpose of a debriefing is to promote participant reflective thinking by allowing the participants to think about and clarify actions that occurred during the simulation (Box 29-3).42 Feedback is provided to the participants by the facilitator to ensure that concepts are understood and the participants are given the right “take-home message” to incorporate into their professional practice. The debriefing process has been reported as the most important component of simulation because of the learning that occurs when concepts are clarified.42–44 Literature suggests that debriefing should last at least as long as the simulation scenario but current practices range from half as
- 22. long as the simulation scenario to twice as long as the scenario.45 Box 29-3 Sample Debriefing Questions for a Pediatric Patient in Isolation for Pneumonia with Cystic Fibrosis Ask at least one question from each section. Aesthetic Questions “I would like each of you to talk to me about the problems _________ was experiencing today.” “What was your main objective during this simulation?” “How did patient safety and isolation issues affect the patient care you provided?”(scenario specific) Personal Questions “Was there any point during the scenario when you felt unsure of your decisions? If yes, how did you manage your feelings and focus on the patient's needs?” “What made you choose the actions, interventions, and focus that you chose for _________?” Empirical Question “I would like each of you to talk with me about the knowledge, skills, attitudes (KSA), and previous experiences that provided you with the ability to provide evidence-based care to _________.” Ethical Question “Talk to me about how your personal beliefs and values influenced the care provided to _________.” Reflection Questions “Please tell me how you knew what to do for a cystic fibrosis
- 23. patient with pneumonia in isolation and why.” “If we could repeat this scenario now, what would you change and why?” “How will you use this in your professional practice?” Standard VII: Evaluation of Expected Outcomes The evaluation and assessment of the participants' performance during the simulation should be based on the focus and desired outcomes of the simulation scenario. The participants should be aware of the evaluation or assessment methods being used before beginning the simulation.35,46,47 While there is growing interest in adoption of clinical simulation within educational programs, there is a gap in empirical research identifying valid and reliable tools to evaluate simulation effectiveness, especially in translating knowledge and skills from simulation experiences to actual clinical practice; research is needed.36,48,49 Also, the National Council of State Boards of Nursing (NCSBN) is conducting a longitudinal national simulation study to determine the appropriate use of simulation for best student outcomes.50 Types of evaluations are skills checklists, formative assessment of performance, or summative evaluation. Skills checklists may be used during a skills validation, such as an indwelling catheter or chest tube insertion for students or an endotracheal intubation for respiratory therapy students. Formative assessments measure a participant's progress toward overall or long-term program objectives. This type of assessment provides the participant with feedback that will aid in professional growth and promote self-reflection. Summative evaluations are traditionally measured at the end of a learning experience, to correlate with the end of the course or program. This type of evaluation may have a grade assigned or use another method to determine student progression. An example of a summative evaluation is an objective structured clinical examination (OSCE). An OSCE summative evaluation can be a graduate student's evaluation at the end of the advanced assessment course to determine his or her ability to
- 24. perform in a traditional clinical setting. Some medical boards require an OSCE to become certified. Regardless of the type of evaluation, the instrument used should have reported psychometric data demonstrating reliability and validity. The evaluation tools currently used in simulation were described in a review by Kardong-Edgren and colleagues and were categorized within the cognitive, psychomotor, and affective learning domains.51 The cognitive domain focuses on application with thinking such as perform, identify, maintain, communicate, prioritize, and provide. An example is that the participant will be able to identify the signs and symptoms of congestive heart failure and provide appropriate interventions for best patient outcomes. The psychomotor domain focuses on the precision of performing the assessment or skill, such as insertion of an intravenous catheter and effective therapeutic communication using Situation-Background-Assessment- Recommendation (SBAR) communication. The affective domain reflects the emotion of reflective thinking by responses to and prioritization of patient care (Box 29-4). Box 29-4 Learning Domains Cognitive domain. Simulation evaluation tools included the Basic Knowledge Assessment Tool 6 (paper-and-pencil test); the Outcome Present State Test Model for Debriefing (worksheets that participants complete during the structured debriefing); the Lasater Clinical Judgment Rubric, based on Tanner's Clinical Judgment Model for student evaluation during simulation; and the Simulation Evaluation Instrument, developed to evaluate the American Association of Colleges of Nursing core competencies for undergraduate nursing students during simulation. Psychomotor domain. There were no tools identified for the psychomotor domain for simulation that reported validity and reliability testing. Affective domain. The evaluation tools identified in this section were developed to measure student satisfaction and
- 25. perceived effectiveness of the simulated clinical experience. The tools identified included a satisfaction survey, the Emergency Response Performance Tool (ERPT), and the Simulation Design Scale. Other tools were reviewed for group evaluation. The Leighton Clinical Learning Environment Comparison Survey (L-CLECS) was designed to compare how well undergraduate students' learning needs were met in the simulated clinical environment and the traditional clinical environment.52 L-CLECS is one of the tools being used during the current national simulation survey by the NCSBN.50 Validity and reliability evaluation measures have been conducted on this instrument. The Creighton Simulation Evaluation Instrument (C-SEI) is a tool that evaluates simulation experiences by measuring assessment skills.53 C-SEI is the second tool being used in the NCSBN's National Simulation Study and has established reliability and validity.50 The C-SEI tool is designed to be modified to meet the specific outcomes of the simulation. The goal of this tool was to evaluate student assessment skills for improvement. As the assessment skills improve, so will clinical performance. Application of Simulation General Application of Simulation to Education The use of simulation in undergraduate nursing, graduate schools for advanced practice nurses (especially nurse anesthetists), medical schools, and interprofessional education has been well documented in the literature. However, literature is not available for simulation applied to doctoral education. Multiple research studies revealed that students have higher satisfaction with higher levels of fidelity.8,54 However, studies have not shown that high-fidelity simulation increases students' clinical reasoning skills.8 There is a growing body of health literature evaluating the differences in student outcomes using low- and high-fidelity simulation experiences. Multiple studies
- 26. indicated no statistically significant differences in student learning outcomes using traditional pencil-and-paper testing scores compared to varying levels of fidelity teaching strategies.55–59 Some studies have demonstrated a statistically significant difference in students' self-perceived improvements depending on the level of fidelity used in simulation.60–64 The participants of these studies preferred high-fidelity teaching strategies as compared to low-fidelity strategies. Several studies recommend that educators need to compare the level of fidelity when considering cost and short- and long-term participant outcomes.56,57 Some authors have questioned the appropriate evaluation method: an OSCE or a paper-and-pencil test.57,65 However, there have not been consistent results with OSCEs in terms of finding differences in participants' performances to compare acquisition of knowledge and applying that knowledge to clinical practice.55 Application of Simulation to Interprofessional Education Many professional medical organizations stated an increasing need for interprofessional education (IPE), as evidenced by the newly introduced Core Competencies for Interprofessional Collaborative Practice sponsored by the Interprofessional Education Collaborative (IPEC) (Table 29-4).66 IPEC was a collaborative effort between multiple associations, including the AACN, American Association of Colleges of Osteopathic Medicine, American Association of Colleges of Pharmacy, American Dental Education Association, Association of American Medical Colleges, and Association of Schools of Public Health. To improve patient safety, evidence-based practice, translational research, and more IPE opportunities are needed. New teaching strategies have evolved. Some of these are in response to the changing technology that has proliferated over the past 25 years. The strategies include the following: 1.Communication tools such as SBAR for more effective
- 27. professional and interprofessional communication 2.Simulation scenarios to practice skills and techniques, assessment, therapeutic communication, interprofessional collaboration, reflection on actions and inactions of participants, and incorporation of evidence-based practice throughout the curriculum and applying these in simulation 3.Informatics capabilities to improve patient care with point- of-care access to information through handheld devices and electronic health records (EHRs) If the interprofessional members of the healthcare team have access to the pertinent information about a patient, healthcare delivery can be more holistic and potentially decrease harm to the patient. Health sciences students can learn the roles and responsibilities of other healthcare team members for collaborative purposes through IPE simulations to ensure the best patient outcomes. For graduate school students, IPE simulations are an excellent way to learn how to function and adapt practices to achieve the best outcomes. TABLE 29-4 Core Competencies for Interprofessional Collaborative Practice CORE COMPETENCY FOCUS APPLICATION WITH SIMULATION OPPORTUNITY FOR IPE Roles and responsibilities for collaborative practice Use the knowledge of each profession's role to assess and address the populations served Demonstrate collaboration of team members in a scenario to clearly communicate with each other and provide the best holistic care to meet the needs of the individual or population
- 28. • Disaster drill simulation • Prehospital injury requiring ambulance transport to the emergency department Interprofessional communication Communicate in a team approach with individuals, families, and communities in a responsive and responsible manner to support well-being and quality of life 1. Communicate with confidence, clarity, and respect to promote understanding of information and management of issues 2. Actively listen and encourage sharing or input from others 3. Recognize one's uniqueness and role within the team and contribute to effective communication, conflict resolution, and positive interprofessional working relationships Scenarios that require multiple professions in diagnosis and planning the care of a patient: • Code situation • Respiratory decline of patient with unknown etiology Interprofessional teamwork and team-based service Apply relationship-building values and the principles of team dynamics to perform effectively in different team roles to plan and deliver services that are safe, timely, efficient, effective, and equitable
- 29. 1. Work with others to develop consensus on the ethical principles to guide all aspects of interaction with individuals and teamwork 2. Use process improvement strategies 3. Reflect on individual and team performance for individual as well as team performance improvement • Home health scenario that requires collaboration via phone • Focus the debriefing process on improvement of any interprofessional simulation Values and ethics for interprofessional practice Work with individuals of other professions to maintain a climate of mutual respect and shared values 1. Provide care for the community 2. Demonstrate high standards of ethical conduct 3. Act with honesty and integrity in relationships with all team members and clients 4. Maintain competence in one's profession Complex scenarios that include moral or ethical decision making and counseling with the patient or family: • Organ transplant decisions • Hospice care • Cultural themes IPE, Interprofessional education. Simulation is a strategy to assist team members with effective communication and promote collaboration with other
- 30. professionals. According to an INACSL survey in 2010, only about half of the respondents provided any IPE. Of the programs providing IPE experiences, only a few institutions stated that the practice was used more than occasionally in the simulation community.44 Challenges to this type of education exist. In particular, the logistics of scheduling multiple professions for simulation is one of the major obstacles for IPE experience.67–70 The Institute of Medicine (IOM) also called for the federal government and professional organizations to study the approaches and foci to determine their contribution to improving the workforce.21,22 The professional organizations have a responsibility to determine the best resources and methods for improving the education of the healthcare workforce, both in initial education and in continuing professional development. Example The following scenario was used in a doctorate of nursing practice program to evaluate nurse practitioner students' ability to assess and develop a differential diagnosis with a patient presenting with angina. Students participated in this experience at the end of their clinical diagnostics course and this was used for summative evaluation purposes. Prior to any simulation experience, a curricular simulation integration form was used to document objectives, evaluation measures, and the specific details related to the scenario (Fig. 29-2). This plan mapped out the specific details related to the simulation experience and contributed to a successful simulation experience for both the faculty and the students. To prepare, the students received the evaluation rubric to review prior to entering the simulation lab for testing (Fig. 29-3). FIG 29-2 Simulation integration and planning form. ASA, Acetylsalicylic acid; BP, blood pressure; DNP, doctor of nursing practice; HTN, hypertension; NP, nurse practitioner; prn, as needed; SL NTG, sublingual nitroglycerin; SOAP,
- 31. subjective, objective, assessment, and plan; SOB, shortness of breath. (Developed by C. Ross, PhD, RN, and V. Howard, EdD, RN. Courtesy of RMU Regional RISE Center.) FIG 29-3 Student evaluation rubric. BP, Blood pressure; NP, nurse practitioner; PVC, premature ventricular contraction; RR, respiratory rate; SOAP, subjective, objective, assessment, and plan. The detailed evaluation rubric (Fig. 29-4) was used by the faculty member to evaluate the students and provide summative feedback. After the scenario the students completed a Scenario Evaluation Form to evaluate the quality of the learning experience (Fig. 29-5).7 These evaluation data were reviewed by the simulation facilitators after the scenario activity to ensure that the scenario met the needs of the students and reflected the highest quality and evidence. Simulation Resources Organizations INACSL was founded after discussions by several attendees of the annual Learning Resource Center Conference in 2001. The nonprofit organization has grown to more than 1500 members worldwide. The organization's mission statement is to promote research and disseminate evidence-based standards for clinical simulation methodologies and learning environments. Its vision is to be nursing's portal to the world of clinical simulation pedagogy and learning environments. The majority of members are nurses, although anyone is welcome to become a member. Institutional membership is also available. The organization is affiliated with SSH and a founding member of the Global Network for Simulation in Healthcare (GNSH), an organization composed of the leadership of simulation organizations worldwide. SSH was founded in 2004 and has a membership of approximately 3000 healthcare providers in all specialty areas. SSH began offering a program to accredit simulation
- 32. laboratories in 2010. The most recent benefit offered by SSH is the ability to receive certification as a simulation educator. Box 29-5 lists additional organizations that support simulation in health education. Leaders There are many experts in the field of simulation; however, some deserve special recognition for the work they have done to further the use of this teaching modality. Asmund S. Laerdal may be the most recognized name in simulation, as he was the founder of the Laerdal Company, now known as Laerdal Medical. Initially making partial and full mannequins to further the education of cardiopulmonary resuscitation FIG 29-4 Detailed faculty evaluation rubric. JVD, jugular venous distention; PQRST, provokes, quality, radiates, severity, time; SOAP, subjective, objective, assessment, and plan. FIG 29-5 Simulation evaluation. DNP, Doctor of nursing practice. (Developed by V. Howard. 2010. Courtesy of RMU Regional RISE Center.) the company branched out into mannequins and supplies for all areas of patient simulation. Dr. J.S. Gravenstein from the University of Florida led the team that created the Human Patient Simulator (HPS), the first and only full-body simulator that responded to gas inhalation, making it an appropriate tool for anesthesia education. Dr. David M. Gaba, Associate Dean for Immersive and Simulation-based Learning at Stanford University School of Medicine, has experience and opinions regarding patient simulation that are sought after by clinicians worldwide. Pamela Jeffries, PhD, RN, contributed the first framework for the development of simulation experiences through her work with the NLN and Laerdal. All of these leaders have made significant contributions to the education of clinicians, including graduate nurses. There are many others
- 33. whose expertise and contributions could also be mentioned here. Box 29-5 U.S. Organizations That Support Simulation in Health Education International Nursing Association for Clinical Simulation and Learning (INACSL): www.inacsl.org Society for Simulation in Healthcare (SSH): www.ssih.org National League for Nursing (NLN): www.nln.org American Association of Colleges of Nursing (AACN): www.aacn.nche.edu The Joint Commission (TJC): www.jointcommission.org Institute of Medicine (IOM): www.iom.edu National Council of State Boards of Nursing (NCSBN): www.ncsbn.org Agency for Healthcare Research and Quality (AHRQ): www.ahrq.gov Conclusion and Future Directions The use of simulation is rapidly emerging as a preferred way to train healthcare professionals in a safe, controlled manner with no risk to patients. One of the reasons for its emergence is that simulation can ameliorate current barriers with traditional clinical experiences. There is a shortage of clinical sites, patients can have complex conditions that a novice learner is unprepared to manage, and clinical sites may have limited student experiences for EHRs, administering medications to pediatric patients, and other situations. These factors, combined with a nursing and nurse educator shortage and the aging population, will further increase the need to teach healthcare providers in a simulation environment. Newer approaches that reflect the advances in technology are virtual reality computer-based simulations and gaming. Gaming is a type of simulation technique that meets the needs of millennial learners. However, this new approach has not yet been as fully developed as the approaches discussed in this chapter. The emergence of technology for educational purposes
- 34. creates a need for faculty and health science educators to understand how to not only operate the technology but also implement it within the academic and service settings while still using sound academic principles. Standards of Best Practice: Simulation will continue to serve as a foundation for all types of simulation-based teaching methodologies. A potential future step is the integration of EHRs into simulation experiences. Simulation experiences that include EHRs are less common and only a few simulation centers have embedded EHRs and other clinical information systems. In the future the entire suite of technical experiences will be available in a simulation center experience. References 1. International Nursing Association for Clinical Simulation and Learning Board of Directors: Standards of best practice: simulation. Clinical Simulation in Nursing. 7(4S), 2011, S1–S2. 2. Benner, P: From Novice to Expert: Excellence and Power in Clinical Nursing Practice . 1984, Addison-Wesley, Menlo Park, CA. 3. Kolb, DA: Experiential Learning . 1984, Prentice Hall, Englewood Cliffs, NJ. 4. Robinson-Smith, G, Bradley, P, Meakim, C: Evaluating the use of standardized patients in undergraduate psychiatric nursing experiences. Clinical Simulation in Nursing. 5(6), 2009, e203– e211, doi:10.1016/j.ecns.2009.07.001. 5. Maran, NJ, Glavin, RJ: Low- to high-fidelity simulation: a continuum of medical education. Med Educ. 37(Suppl 1), 2003, 22–28. 6. Alinier, G: A typology of educationally focused medical simulation tools. Med Teach. 29(8), 2007, 1–8,
- 35. doi:10.1080/01421590701551185. 7. Howard, V, Ross, C, Mitchell, A, Nelson, G: Human patient simulators and interactive case studies: a comparative analysis of learning outcomes and student perceptions. Comput Inform Nurs. 28(1), 2010, 42–48. 8. Lapkin, S, Levett-Jones, T, Bellchambers, H, Fernandez, R: Effectiveness of patient simulation manikins in teaching clinical reasoning skills to undergraduate nursing students: a systematic review. Clinical Simulation in Nursing. 6(6), 2010, e207–e222, doi:10.1016/j.ecns.2010.05.005. 9. McGaghie, W, Issenberg, SB, Petrusa, E, Scalese, R: A critical review of simulation-based medical education research: 2003– 2009. Med Educ. 44, 2009, 50–63. 10. Kameg, K, Howard, V, Clochesy, J, Mitchell, AM, Suresky, J: Impact of high fidelity human simulation on self-efficacy of communication skills. Issues Ment Health Nurs. 31(5), 2010, 315–323. 11. Cooper, S, Cant, R, Porter, J, et al.: Simulation based learning in midwifery education: a systematic review. Women Birth. 25(2), 2011, 64–78, doi:10.1016/j.wombi.2011.03.004. 12. Kirkpatrick, DL, Kirkpatrick, JD: Evaluating training programs. 3rd ed, 2006, Berrett-Koehler Publishers, San Francisco, CA. 13. Barsuk, JH, McGaghie, WC, Cohen, ER, Balachandran, JS, Wayne, DB: Use of simulation-based mastery learning to improve the quality of central venous catheter placement in a medical intensive care unit. J Hosp Med. 4(7), 2009, 397–403, doi:10.1002/jhm.468. 14. Draycott, T, Crofts, J, Ash, J, et al.: Improving neonatal
- 36. outcome through practical shoulder dystocia training. Obstet Gynecol. 112(1), 2008, 14–20. 15. McCarthy, J: Malpractice insurance carrier provides premium incentive for simulation-based training and believes it has made a difference. Anesthesia Patient Safety Foundation Newsletter. 2007, http://www.apsf.org/newsletters/html/2007/spring/17_malpracti ce.htm. 16. Kotter, JP: Leading Change . 1996, Harvard Business Review Press, Boston, MA. 17. Gantt, L: Strategic planning for skills and simulation labs in colleges of nursing. Nurs Econ. 28(5), 2010, 308–313. 18. Kneebone, R: Evaluating clinical simulations for learning procedural skills: a theory-based approach. Acad Med. 80(6), 2005, 549–553. 19. Cronenwett, L, Sherwood, G, Barnsteiner, J, et al.: Quality and safety education for nurses. Nurs Outlook. 55(3), 2007, 122– 131. 20. Institute of Medicine (IOM): Crossing the Quality Chasm: A New Health System for the 21st Century . 2001, National Academies Press, Washington, DC. 21. Institute of Medicine (IOM): Health Professions Education: A Bridge to Quality . 2003, National Academies Press, Washington, DC. 22. Wachter, RM: The end of the beginning: patient safety five years after “to err is human.”. Health Affair. 2004, W4-534-545 http://content.healthaffairs.org/content/early/2004/11/30/hlthaff .w4.534.short.
- 37. 23. Clapper, TC: Beyond Knowles: what those conducting simulation need to know about adult learning theory. Clinical Simulation in Nursing. 6(1), 2010, e7–e14, doi:10.1016/j.ecns.2009.07.003. 24. Onda EL. Situated cognition: its relationship to simulation in nursing education. Clinical Simulation in Nursing. In press. doi:10.1016/j.ecns.2010.11.004. 25. Paige, JB, Daley, BJ: Situated cognition: a learning framework to support and guide high-fidelity simulation. Clinical Simulation in Nursing. 5(3), 2009, e97–e103, doi:10.1016/j.ecns.2009.03.120. 26. Knowles, MS: Andragogy, not pedagogy. Adult Leadership. 16(10), 1968, 350–352, 386. 27. Knowles, MS: The Adult Learner: A Neglected Species. 3rd ed, 1984, Gulf, Houston, TX. 28. Kolb, DA: Organizational Behavior: An Experiential Approach to Human Behavior in Organizations . 1995, Prentice Hall, Englewood Cliffs, NJ. 29. Waldner, MH, Olson, JK: Taking the patient to the classroom: applying theoretical frameworks to simulation in nursing education. Int J Nurs Educ Scholarsh. 4(1), 2007, 1–14. 30. Lasater, K: High-fidelity simulation and the development of clinical judgment: students’ experience. J Nurs Educ. 46(6), 2007, 269–276. 31. Lasater, K: Clinical judgment development: using simulation to create an assessment rubric. J Nurs Educ. 46(11), 2007, 498– 503.
- 38. 32. Jeffries, PR: Preface. In Jeffries, PR (Ed.): Simulation in Nursing Education: From Conceptualization to Evaluation. 2007, National League for Nursing, New York, NY, xi–xii. 33. Gaba, DM: The future vision of simulation in health care. Qual Saf Health Care. 13, 2004, i2–i10, doi:10.1136/qshc.2004.009878. 34. Clark, CC: Classroom Skills for Nurse Educators . 2008, Jones and Bartlett, Sudbury, MA. 35. Decker, S, Gore, T, Feken, C: Simulation. In Bristol, T, Zerwehk, J (Eds.): Essentials of e-Learning for Nurse Educators. 2011, FA Davis, Philadelphia, PA, 277–294. 36. Howard, VM, Englert, N, Kameg, K, Perozzi, K: Integration of simulation across the undergraduate curriculum: student and faculty perspectives. Clinical Simulation in Nursing. 7(1), 2011, e1–e10, doi:10.1016/j.ecns.2009.10.004. 37. International Nursing Association for Clinical Simulation and Learning Board of Directors: Standard I: terminology. Clinical Simulation in Nursing. 7(4S), 2011, S3–S7, doi:10.1016/j.ecns.2011.05.005. 38. International Nursing Association for Clinical Simulation and Learning Board of Directors: Standard II: professional integrity of participants. Clinical Simulation in Nursing. 7(4S), 2011, S8–S9, doi:10.1016/j.ecns.2011.05.006. 39. International Nursing Association for Clinical Simulation and Learning Board of Directors: Standard III: participant objectives. Clinical Simulation in Nursing. 7(4S), 2011, S10– S11, doi:10.1016/jecns.2011.05.007. 40.
- 39. International Nursing Association for Clinical Simulation and Learning Board of Directors: Standard IV: facilitation methods. Clinical Simulation in Nursing. 7(4S), 2011, S12–S13, doi:10.1016/j.ecns.2011.05.008. 41. International Nursing Association for Clinical Simulation and Learning Board of Directors: Standard V: simulation facilitator. Clinical Simulation in Nursing. 7(4S), 2011, S14–S15, doi:10.1016/j.ecns.2011.05.009. 42. International Nursing Association for Clinical Simulation and Learning Board of Directors: Standard VI: the debriefing process. Clinical Simulation in Nursing. 7(4S), 2011, S16–S17, doi:10.1016/j.ecns.2011.05.010. 43. Childs, J, Sepples, S: Clinical teaching by simulation: lessons learned from a complex patient care case scenario. Nursing Education Perspectives. 27(3), 2006, 154–158. 44. Gore, T, Van Gele, P, Ravert, P, Mabire, C: A 2010 survey of the INACSL membership about simulation use. Clinical Simulation in Nursing. 8(4), 2012, e125–e133, doi:10.1016/j.ecns.2012.01.002. 45. Waxman, KT: The development of evidence-based clinical simulation scenarios: guidelines for nurse educators. J Nurs Educ. 49(1), 2010, 29–35. 46. International Nursing Association for Clinical Simulation and Learning Board of Directors: Standard VII: evaluation of expected outcomes. Clinical Simulation in Nursing. 7(4S), 2011, S18–S19, doi:10.1016/j.ecns.2011.05.011. 47. Jeffries, PR, McNelis, AM: Evaluation. In Nehring, WM, Lashley, FR (Eds.): High-Fidelity Patient Simulation in Nursing Education. 2010, Jones and Bartlett, Boston, MA, 405–424.
- 40. 48. Hayden, J: Use of simulation in nursing education: national survey results. Journal of Nursing Regulation. 1(3), 2010, 52– 57. 49. Kardong-Edgren, S, Willhaus, J, Bennett, D, Hayden, J: Results of the National Council of State Boards of Nursing National Simulation Survey: Part II. Clinical Simulation in Nursing. 8(4), 2012, e117–e123, doi:10.1016/j.ecns.2012.01.003. 50. National Council of State Boards of Nursing (NCSBN): NCSBN National Simulation Study NCSBN https://www.ncsbn.org/2094.htm, 2011. 51. Kardong-Edgren, S, Adamson, KA, Fitzgerald, C: A review of currently published evaluation instruments for human patient simulation. Clinical Simulation in Nursing. 6(1), 2010, e25– e35, doi:10.1016/j.ecns.2009.08.004. 52. Leighton, KL: Clinical learning environment comparison survey. Paper AAI3271929 In Learning Needs in the Traditional Clinical Environment and the Simulated Clinical Environment: A Survey of Undergraduate Nursing Students [doctoral dissertation]. 2007, University of Nebraska–Lincoln, Lincoln, NE. 53. Todd, M, Manz, JA, Hawkins, KS, Parsons, ME, Hercinger, M: The development of a quantitative evaluation tool for simulations in nursing education. Int J Nurs Educ Scholarsh. 5(1), 2008, Article 41 http://www.bepress.com/ijnes/vol5/iss1/art41/. 54. Jeffries, P, Rizzolo, M: NLN/Laerdal Project Summary Report, Designing and Implementing Models for the Innovative Use of Simulation to Teach Nursing Care of Ill Adults and Children: A National Multi-Site Study . 2006, National League for Nursing,
- 41. New York, NY. 55. De Giovanni, D, Roberts, T, Norman, G: Relative effectiveness of high- versus low-fidelity simulation in learning heart sounds. Med Educ. 43(7), 2009, 661–668. 56. Friedman, Z, Siddiqui, N, Katznelson, R, Devito, I, Bould, MD, Naik, V: Clinical impact of epidural anesthesia simulation on short- and long-term learning curve: high- versus low-fidelity model training. Reg Anesth Pain Med. 34(3), 2009, 229–232. 57. Kardong-Edgren, S, Lungstrom, N, Bendel, R: VitalSim versus SimMan: a comparison of BSN student test scores, knowledge retention, and satisfaction. Clinical Simulation in Nursing. 5(3), 2009, e105–e111, doi:10.1016/j.ecns.2009.01.007. 58. Kinney, S, Henderson, D: Comparison of low fidelity simulation learning strategy with traditional lecture. Clinical Simulation in Nursing. 4(2), 2008, e15–e18, doi:10.1016/j.ecns.2008.06.005. 59. Lee, KHK, Grantham, H, Boyd, R: Comparison of high- and low-fidelity mannequins for clinical performance assessment. Emerg Med Australas. 20(6), 2008, 508–514. 60. Faran, JM, Paro, JAM, Rodriguez, RM, et al.: Hand-off education and evaluation: piloting the observed simulated hand- off experience (OSHE). J Gen Intern Med. 25(2), 2010, 129– 134. 61. Ham, K, O'Rourke, E: Clinical preparation for beginning nursing students. Nurse Educ. 29(4), 2004, 139–141. 62. Hoadley, T: Learning advanced cardiac life support: a comparison study on the effects of low- and high-fidelity simulation. Nurs Educ Perspect. 30(2), 2009, 91–95. 63.
- 42. Radhakrishnan, K, Roche, JP, Cunningham, H: Measuring clinical practice parameters with human patient simulation: a pilot study. Int J Nurs Educ Scholarsh. 4(1), 2007, 1–11. 64. Tiffen, J, Corbridge, S, Shen, BC, Robinson, P: Patient simulator for teaching heart and lung assessment skills to advanced practice nursing students. Clinical Simulation in Nursing. 7(3), 2010, e91–e97, doi:10.1016/j.ecns.2009.10.003. 65. Kardong-Edgren, S, Anderson, M, Michaels, J: Does simulation fidelity improve student test scores?. Clinical Simulation in Nursing. 3(1), 2007, e21–e24, doi:10.1016/j.ecns.2009.05.035. 66. Interprofessional Education Collaborative Expert Panel: Core Competencies for Interprofessional Collaborative Practice: Report of an Expert Panel . 2011, Interprofessional Education Collaborative, Washington, DC. 67. Alinier, G: Enhancing trainees’ learning experience through the opening of an advanced multiprofessional simulation training facility at the University of Hertfordshire. British Journal of Anaesthetic and Recovery Nursing. 8(2), 2007, 22–27. 68. Angelini, DJ: Interdisciplinary and interprofessional education: what are the key issues and considerations for the future?. J Perinat Neonatal Nurs. 25(2), 2011, 175–179. 69. Leonard, B, Shuhaibar, EL, Chen, R: Nursing student perceptions of intraprofessional team education using high- fidelity simulation. J Nurs Educ. 4(11), 2010, 628–631, doi:10.3928/01484834-20100730-06. 70. Reese, CE, Jeffries, PR, Engum, SA: Learning together: using simulations to develop nursing and medical student collaboration. Nurs Educ Perspect. 31(1), 2010, 33–37. Discussion Questions
- 43. 1. You are a graduate teaching assistant at the local university. A faculty member approaches you to “do” a simulation for class. What information do you need prior to developing the simulation? Provide a rationale for the information needed. 2. As a faculty member facilitating a debriefing, list five questions that you would ask to promote self-reflection. 3. Provide an example of an interprofessional simulation that would facilitate your graduate-level education. List the specific learning objectives, the team members, the participants' experience level and learning, and the type of facilitation and debriefing to guide this simulation scenario. 4. You are a faculty member struggling with generating support for your simulation program. You are experiencing resistance from faculty members and administration with the implementation of this new technology. What can you do to enhance buy-in? Case Study You have been hired to teach in a graduate health program. Your newly developed course has an objective that states: Upon completion of this course, the learner will be able to demonstrate interprofessional team building concepts. As a new educator, you would like to include simulation as a teaching methodology. After you are hired, you find a rarely used, high-fidelity Human Patient Simulator in the corner of your skills lab. You inquire about using it for your course but are met with resistance from other faculty members, who tell you that “there is no reason to use simulation. We've always taught our content using written case scenarios and we're doing just fine.” Discussion Questions 1. Use Kotter's eight steps leading to successful change to develop a plan to implement simulation for teaching team
- 44. concepts. 2. What information should you incorporate when developing the scenario? 3. Unfortunately, students who experienced the scenario at 8 a.m. are sharing information with students scheduled later in the day. Which INACSL standard addresses this issue and how can you deter this behavior? 4. Which published document can assist you in clarifying interprofessional competencies? Pageburst Integrated Resources Chapter 29 Simulation in Healthcare Education Valerie Howard Kim Leighton Teresa Gore The emergence of technology for educational purposes creates a need for faculty and health science educators to understand how to not only operate the technology but also implement it within the academic and service settings while still using sound aca demic principles. Objectives At the completion of this chapter the reader will be prepared to:
- 45. 1.Define the different types of simulation modalities available 2.Describe the challenges and opportunities inherent to simulation 3.Apply the Stan dards of Best Practice: Simulation to the simulation lab 4.Discuss the use of simulation - based education in interprofessional experiences 5.Analyze the similarities and differences related to the available simulation resources 6.Develop evidenc e - based simulation activities for graduate - level education Key Terms Clinical scenario, 459 Debriefing, 461 Fidelity, 455
- 46. Learning environment, 457 Simulation, 454 Simulation experience, 457 Standards of Best Practice: Simulation, 460 Abstract The use of simulated learning experiences has rapidly emerged in healthcare education as a method of training healthcare providers in a safe environment without subjecting patients to harm. Multiple definitions of simulation - related terms exist, so the importance of the use of standardized terminology is Chapter 29 Simulation in Healthcare Education Valerie Howard Kim Leighton Teresa Gore The emergence of technology for educational purposes creates a need for faculty and health science educators to understand how to not only operate the technology but also implement it within the academic and service settings while still using sound academic principles. Objectives At the completion of this chapter the reader will be prepared to: 1.Define the different types of simulation modalities available 2.Describe the challenges and opportunities inherent to
- 47. simulation 3.Apply the Standards of Best Practice: Simulation to the simulation lab 4.Discuss the use of simulation-based education in interprofessional experiences 5.Analyze the similarities and differences related to the available simulation resources 6.Develop evidence-based simulation activities for graduate- level education Key Terms Clinical scenario, 459 Debriefing, 461 Fidelity, 455 Learning environment, 457 Simulation, 454 Simulation experience, 457 Standards of Best Practice: Simulation, 460 Abstract The use of simulated learning experiences has rapidly emerged in healthcare education as a method of training healthcare providers in a safe environment without subjecting patients to harm. Multiple definitions of simulation-related terms exist, so the importance of the use of standardized terminology is PAGE 471 Discussion Questions 1. You are a graduate teaching assistant at the local university. A faculty member approaches you to “do” a simulation for class. What information do you need prior to developing the simulation? Provide a rationale for the information needed.
- 48. Case Study You have been hired to teach in a graduate health program. Your newly developed course has an objective that states: Upon completion of this course, the learner will be able to demonstrate interprofessional team building concepts. As a new educator, you would like to include simulation as a teaching methodology. After you are hired, you find a rarely used, high-fidelity Human Patient Simulator in the corner of your skills lab. You inquire about using it for your course but are met with resistance from other faculty members, who tell you that “there is no reason to use simulation. We've always taught our content using written case scenarios and we're doing just fine.” Discussion Questions 1. Use Kotter's eight steps leading to successful change to develop a plan to implement simulation for teaching team concepts. PAGE 471 Discussion Questions 1. You are a graduate teaching assistant at the local university. A faculty member approaches you to “do” a simulation for class. What information do you need prior to developing the simulation? Provide a rationale for the information needed. Case Study
- 49. You have been hired to teach in a graduate health program. Your newly developed course has an objective that states: Upon completion of this course, the learner will be able to demonstrate interprofessional team building concepts. As a new educator, you would like to include simulation as a teaching methodology. After you are hired, you find a rare ly used, high - fidelity Human Patient Simulator in the corner of your skills lab. You inquire about using it for your course but are met with resistance from other faculty members, who tell you that “there is no reason to use simulation. We've always taught our content using written case scenarios and we're doing just fine.” Discussion Questions 1. Use Kotter's eight steps leading to successful change to develop a plan to implement simulation for teaching team concepts. PAGE 471 Discussion Questions 1. You are a graduate teaching assistant at the local university. A faculty member approaches you to “do” a simulation for class. What information do you need prior to developing the simulation?
- 50. Provide a rationale for the information needed. Case Study You have been hired to teach in a graduate health program. Your newly developed course has an objective that states: Upon completion of this course, the learner will be able to demonstrate interprofessional team building concepts. As a new educator, you would like to include simulation as a teaching methodology. After you are hired, you find a rarely used, high-fidelity Human Patient Simulator in the corner of your skills lab. You inquire about using it for your course but are met with resistance from other faculty members, who tell you that “there is no reason to use simulation. We've always taught our content using written case scenarios and we're doing just fine.” Discussion Questions 1. Use Kotter's eight steps leading to successful change to develop a plan to implement simulation for teaching team concepts.