Biliary Tract Cancer Types, Risk Factors, Diagnosis and Treatment
•Download as PPTX, PDF•
21 likes•4,425 views

This document discusses biliary tract cancers including cholangiocarcinoma and gallbladder cancer. It provides information on risk factors, pathogenesis, clinical presentation, diagnostic evaluation, staging systems, and treatment options. Biliary tract cancers are generally diagnosed at late stages and have a poor prognosis. Surgical resection remains the only potentially curative treatment option, but palliative approaches are used for non-resectable disease.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Biliary Tract Cancer Types, Risk Factors, Diagnosis and Treatment
Similar to Biliary Tract Cancer Types, Risk Factors, Diagnosis and Treatment (20)
More from Dalia Cosio Benson
Recently uploaded
Recently uploaded (20)
Biliary Tract Cancer Types, Risk Factors, Diagnosis and Treatment
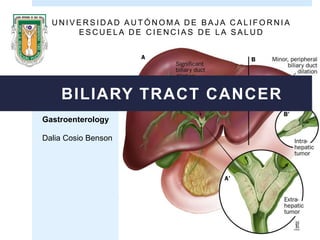
- 1. Gastroenterology Dalia Cosio Benson BILIARY TRACT CANCER U N I V E R S I D A D A U T Ó N O M A D E B A J A C A L I F O R N I A E S C U E L A D E C I E N C I A S D E L A S A L U D
- 2. Carcinoma of intrahepatic and extrahepatic bile ducts Gallbladder carcinoma Carcinoma of the ampulla Biliary malignancies are divided into three general categories :
- 3. In the US and other Western countries biliary malignancies are rare. Biliary cancers are highly aggressive and have a poor prognosis. They are generally resistant to chemotherapy
- 4. CHOLANGIOCARCINOMA Comes from cells of the bile ducts, both inside and outside the liver. The term bile duct cancer is also used synonymously . This type of cancer is slightly more common in men than in women ( 1.3: 1.0) and usually affects patients of 50-70 years >
- 5. Hepatobiliar cancer subtype Frequency % HCC 84 Cholangiocarcinoma 13 Cholangiocellular and fibrolamellar 2 Angiosarcoma, sarcoma, hepatoblastoma 1 Relative frequency of hepatobiliary tumors diagnosed (USA)
- 6. About 8,000 new cases of gallbladder and bile duct cancer are diagnosed annually in the US . These cancers account for 15-20% of cases of primary hepatobiliary malignancies. > 2.5 to 1 Gallbladder carcinoma They are more frequently diagnosed at 60 or 70 years old
- 7. Cholangiocarcinomas are classified into intrahepatic or extrahepatic hilar distal . It is 9a gastroenterology malignancy common. The global incidence of cholangiocarcinoma is heterogeneous. Highest incidence is observed in Southeast Asia , with 96 cases per 100,000 population Lowest incidence iobserved in Australia , with 0.1 cases per 100,000 population . Intrahepatic cholangiocarcinoma is the 2nd most common primary malignancy liver
- 8. GLOBAL INCIDENCE OF GALLBLADDER CANCER G L O B O C A N 2 0 1 2 ( I A R C ) Incidence rate per 100,000 population Both sexes , all ages
- 9. GLOBAL MORTALITY OF GALLBLADDER CANCER G L O B O C A N 2 0 1 2 ( I A R C ) Incidence rate per 100,000 population Both sexes , all ages
- 10. The relative risk of carcinoma is 2.4 times higher for patients with calculations of 2.0 to 2.9 cm and 10 times more in patients with stones > 3.0 cm in diameter. Cholelithiasis - cholecystitis chronic Gallbladder carcinoma Cholecystitis chronic Polyposis coli Malignant transformation Gallbladder cancer
- 12. GALLBLADDER CANCER Cholelithiasis (gallstones) Salmonella tiphy o parathypi (chronic carrier) Inflammatory bowel disease Genetic predisposition Obesity Chronic cholecystitis, (chronic mucosal damage) Polypoid lesions in the bladder, adenomiomatosis ¿? Autoimmune disease ( primary biliary cirrhosis, primary sclerosing colangisits , inflammatory bowel disease) Exposure to carcinogenic Porcelain gallbladder
- 13. CHOLANGIOCARCINOMA Major risk factors: chronic inflammation Parasitic infections(Clonorchis sinensis, Opisthorchis viverrini) Autoimmune disease ( primary biliary cirrhosis, primary sclerosing colangisits , inflammatory bowel disease) Anatomical abnormalities (biliary atresia, congenital abnormalities of bile ducts) Liver disease cystic Cysts choledocus Some association with cirrhosis, but less than for CCH Carcinogens: thorotrast, oximetalona, nitrosaminas
- 14. BILIARY TRACT CANCER (CHOLANGIOCARCINOMA) • Colangiocitos • Células madre de los canalículos biliares (células de Hering) • Células epiteliales de las glándulas peribiliares Inflammation Microenvironment that promotes malignant transformation of cells associated with ducts Inactivation of DNA repair genes by mismatch and tumor suppresor genes Increases bile acid concentrations Cytokines Growth factors Expression of protooncogenes iNOS ROS
- 16. GALLBLADDER CANCER Gallbladder carcinoma It develops a focus of dysplasia or mucosal carcinoma in situ (CIS) Progresses to adenocarcinomaTime to progression of dysplasia to carcinoma is around Inflammation iNOS COX-2 Mutations in: Gen TP53 (35-92% of gallbladder carcinomas, 86% CIS and 28% focus of dysplasia) Oncogene K-ras (60% gallbladder carcinoma) ROS
- 17. Age (years) 30-40 45 55 60 Normal gallbladder Gallstones and crhonic inflammation Dysplasia Carcinoma in situ Invasive carcinoma Mutationss TP53 Mutationss mDNA Overexpression COX-2 Methylation of promotersTSG Loss of heterozygosity in 3p - 8p Mutations in FHIT and CDKN2A Loss in heterozygosity in 9q, 18q and 22q KRAS mutations
- 18. Most of the cases (90%) are adenocarcinomas. They are hightly desmoplastic tumors paucicelulares Macroscopically can be described according to their growth characteristics: CHOLANGIOCARCINOMA Nodular Infiltative (periductal) Papilar (intraductal) Cholangiocarcinoma intrahepatic or peripheral Cholangiocarcinoma ductal (ducts) Mass-forming type Nodular, infiltrative or papilar
- 20. Cholangiocarcinoma intrahepatic When tumors originate in the liver these can be large or small In contrast, when the tumors arise along the bile ducts in the liver entering, tumors tend to be small
- 23. Extrahepatic Intrahepatic It grows to the 2nd ductal division (branches of the hepatic ducts right of left direction) It grows in the bifurcation of the common hepatic duct of the right or left hepatic ducts. It grows in the extrahepatic bile duct from the bifurcation of the common hepatic duct at the vater ampulla They’re the most common
- 24. BISMUTH-CORLETTE STAGING STAGING TYPE I In the common hepatic duct, lower than the confluence of the hepatic ducts TYPE II In the confluence of the hepatic ducts TYPE IIIa At the confluence with extension to the right hepatic duct TYPE IIIb At the confluence with the extension to the left hepatic duct TYPE IV Extension to both hepatic duct
- 27. 80-90 % of cases are adenocarcinomas: most of these are moderately well differentiated. Among other less common types are anaplastic carcinoma, squamous cell carcinoma and adenosquamous carcinoma. Gallbladder cancer 60% of GBC occur in the fundus 30% occur in the body 10% in the neck Bladder carcinoma proliferates by direct invasion , lymphatic or hematogenous metastasis , perineural invasion, and invasion intraperitoneal or intraductal
- 28. CHOLANGIOCARCINOMA The clinical presentation is not specific and is insufficient to make the diagnosis. At an early stage patients are usually asymptomatic . In more advanced stages, patients usually present: Weightloss Abdominal discomfort Jaundice Hepatomegaly or palpable mass Obstruction of the biliary tract is rare in intrahepatic CCA Tumor -related fever may occur (rare ), however the night sweats are common in advanced disease.
- 29. Evidence of obstructive cholestasis: high levels of alkaline phosphatase (ALP) and bilirubin Serum tumor markers: CA 19-9, carcinoembryonic antígen y CA-125 Laboratory exam The most widely used is the CA-19-9 In patients with CEP sensitivity and specificity for CCA is 79% and 98%. Values of 129 U/mll Imaging studies An essential tool for diagnosis is colangiography: gives anatomical information and material to make the diagnosis. Cholangiopancreatography retrograde endoscopic (CPRE) Cholangiography transhepátic percutaneous (CTH) Cholangiography magnetic resonance (CPRM) TAC: Used primarily for the preoperative plan: provides information of the vascular structures and other anatomical structures that may affect the surgical plan. CHOLANGIOCARCINOMA
- 30. Both techniques give us information intrabiliary extent of the tumor and allow us to obtain a cytological sample and therapeutic intervention. Magnetic resonance cholangiography does not allow us to do an intervention. This is a noninvasive technique that provides additional information extrabiliar extent of the tumor, vascular structure of the primary tumor relationship with surrounding structures, as well as intra- and extrahepatic metastases.
- 34. ALGORITHM PARA FOR DIAGNOSIS (CCA) Estenosis dominante CA 19-9 >129 U/mL Pos. biopsia, citología o FISH polisomia Preocupación mínima clínica Menejo de CCA Observación Niveles de CA 19-9 Colangiografía endoscópica (cepillado, citología, FISH) Indeterminado Sospecha clínica de CCA MRI Negativo Preocupación significativa clínica Escaneo con PET Negativo Estenosis no dominante Neg. biopsia/ citología/citología avanzada CA 19-9 <129 U/mL “Hot spot” Masa Encierre vascular
- 35. CHOLANGIOCARCINOMA Sistema de estadificación de la AJCC The American Joint Committee on Cancer (AJCC) TNM system There are actually 3 different staging systems for bile duct cancers, depending on where they start: • Intrahepatic bile duct cancers (those starting within the liver) • Perihilar (hilar) bile duct cancers (those starting in the hilum, the area just outside the liver) • Distal bile duct cancers (those starting farther down the bile duct system) American Cancer Society. Bile Duct Cancer (Cholangiocarcinoma). 2014
- 36. HILIAR CHOLANGIOCARCINOMA Sistema de estadificación de la AJCC
- 37. The only curative treatment is surgical resection cholangiocarcinoma. Treatment includes surgical resection and liver transplantation (in some cases). Intrahepatic cholangiocarcinoma loners can be resected liver segmentectomy or lobectomy. Palliative treatment.
- 38. A –B surgical technique for unilateral hepatojejunostomy with Roux-en- Y anastomosis and left hepatic lobectomy
- 39. Patel T. Cholangiocarcinoma-controversies and challenges. NRGastro. 2011;8: 189-200.
- 40. INTRAHEPATIC EXTRAHEPATIC American Cancer Society. Bile Duct Cancer (Cholangiocarcinoma). 2014
- 41. GALLBLADDER CANCER 2/3 of cases are diagnosed accidentally during or after cholecystectomy for presumed benign disease. The most common presentations include: The CEA and CA 19-9 markers are most commonly used. Abdominal pain or biliary pain Jaundice secondary invasion of the bile ducts or metastasize to hepatoduodenal ligamentdominal Abdominal distention Loss weight
- 42. Tumos markers: CAE Y CA 19-9 Abdominal ultrasound (is the first to be performed after the patient any symptoms or risk factors mentioned). Early-stage cancers, especially sessile polyps can not be seen. Typical image of gallbladder cancer: Focal or diffuse wall thickening Intraluminal mass >2 cm arising from the gallbladder wall Hepatic mass that replaces or darkens the bladder, commontly invades other organs Indicative findings suggesting that the lesion is malignant: Thickening of the wall (irregular and aymmetrical) >1 cm Nodular intraluminal mass or smooth, >1 cm, fixed to the wall of the bladder, which does not move with the patient's movements and has no acoustic shadow CT and MRI may be useful in the diagnosis if ultrasound findings are indeterminate
- 45. GALLBLADDER CANCER Staging system of AJCC
- 46. INTRA OR POST-OPERATORY DIAGNOSIS POSTOPERATORY DIAGNOSIS OF GALLBLADDER CANCER T2, T3, T4 ESTADIFICACIÓN M1 Tratamiento paliativo No más tratamiento si los márgenes son negativos Colecistectomía radical Resecable T1a T1 Re-exploración T1b No resecable
- 47. Bartlett D, Di Bisceglie A, Dawson L. Cancer of the Liver . En: De Vita, Hellman, Rosenberg. Cancer, principles & practice of oncology. 10th edición. Philadelphia: Lippincot Williams; 2012. p. 1129-1156. Villalobos, J., Valdovinos, Olivera (2012). Gastroenterología. Méndez editores. 6ta edición GLOBOCAN 2012 (IARS). Organización Mundial de la Salud. Phan A. Hepatobiliary malignancies. En: The MD Anderson Manual of Medical Oncology. 2da ed. Mc Graw- Hill: 2011. Ferlman M, Friedman L, Brandt L. Sleisengen and Fordtran’s- Garstrointestinal and liver disease: pathophysiology/diagnosis/management. 9na ed. Philadelphia: Sounders Elservier: 2010. Patel T. Cholangiocarcinoma-controversies and challenges. NRGastro. 2011;8: 189-200 http://www.scielo.org.co/pdf/rcg/v26n2/v26n2a08 .
Editor's Notes
- Estos cánceres representan el 15-20 % de los casos de tumores malignos primarios hepatobiliar
- Los colangiocarcinomas se clasifican en intrahepáticos, hiliares o extrahepáticos distales. Es la 9a malignidad gastroenterológica más común. La incidencia global del colangiocarcinoma es heterogénea. La incidencia más alta se observa en el Sudeste de Asia, con 96 casos por 100,000 habitantes. La incidencia más baja se observa en Australia, con 0.1 casos por 100,000 habitantes.
- EU: el carcinoma de vesicula biliar es el mas comun de los canceres de la via biliar. Pero es raro, incidencia de 1 a 2 por cada 100,000 hab. La incidencia de GBC tambien es alta en nativos americanos, latinos, japoneses y americanos de origen mexicano. Niveles bajos: nigeria, nueva zelanda, maories. *areas urbanas muestra alta incidencia que regiones rurales y se ha sugerido que el nivel socioeconomico bajo tiene tasas mas altas de incidencia, por retrasos en el acceso a la colecistectomia. La incidencia mas alta la tienen en chile y bolivia.
- Alemania y paises bjos tienen una alta mortalidad. En estados unidos, canada ha declinado, estos cambios coinciden con el numero de laparoscopias por colecistectomias realizadas. La mortalidad mas alta la tiene CHILE, es de 5.2% la mas alta en el mundo. GBC es la principal causa de muerte por cancer entre las mujeres en chile.
- Los macanismos que predisponen a este factor de riesgo (colelitiasis) no son conocidos. Colecistolitiasis esta presente en el 70-90% del carcinoma vesicular. Son importantes, la duracion de la enfermedad, la edad del paciente, el tamaño de los calculos biliares, los efectos del proceso de carcinogenesis desarrollados, la composicion quimica, la bacteria implicada. La colecistitis cronica induce polipos adenomatosos?????*
- Metilcolanteno: La exposición se asocia con su uso en la investigación bioquímica (HSDB). También puede estar presente en los contaminantes de aire industrial, el humo de carbón o quemadores de coque, y en el alquitrán del tabaco. **la exposicion a toxicos ambientales en el caucho, textiles, e industrias metalicas, tienen asociacion con GBC. Los quimicos implicados en la carcinogenesis incluyen methyldopa, anticonceptivos orales e izoniazid
- Vesicula en porcelana (calcificacion parcial o total de la pared de la vesicula) esta asociacion es controversial, se reporta una incidencia del 25% -slmonella tiphy esta sociada:por que se sufre de una inflamacion cronica de la vesicula biliar y tienen un sixfold mas alta probabilidad de cancer de vesicula -bilis por HP «sixfold» -obesidad: tambien es un factor de riesgo, paralelo al riesgo de enfermedad calculos biliares. -otras sociaciones: cirugia previa gastrica, enfermedad inflamatoria intestinal, polipos adenomatosos.
- Thorotrast: óxido de torium Oximetalona: esterioide oral muy fuerte, fecto androgénico bastante fuerte, hepatotóxico. Clonorchis sinensis: conocido como duela hepática china (oriental liver fluke), es un gusano parásito (trematodo), vive en hígado humano, principalmente en los conducto biliares y la vesícula biliar y se alimenta de biliar. Es endémica de Japón, China y Taiwan y el sureste de Asia.Pescado crudo, causa cálculos pigmentados Hepatitis C y enfermedad de Caroli
- Colangiocitos: celulas del epitelio de los ductos. Celulas madre, en los conductos de hering: Celulas epiteliales de las glandulas peribiliares: Mismatch: mal-apareamiento Protooncogenes: con sobreactividad, no puede ser controlada de manera normal y no pueden ser reprimidos adecuadamente. O hay una mutacion que resulta en un producto proteico que funciona de manera anormal. En celulas cancerosas mas de un protooncogen esta alterado y su actividad no puede ser controlada. Tienen la actividad de regulacion transcripcional, traduccion, modificacion de proteinas. Estimulan la expresion de otros genes, y regulan el ciclo celular. Estimula a la celula a dividirse
- La progresión a adenocarcinoma es similar a la del cáncer de colon. Al igual que el colangiocarcinoma el factor de riesgo más importantes es la inflamación…. Especies reactivas de oxigeno – mediadas por la regulacion de eNOS E inhibidores de inflamacion COX-2
- Paucicelular: un área de baja densidad celular o celularidad escasa. La gran mayoría corresponden a adenocarcinomas que se caracterizan por la proliferación de estructuras glandulares malignas que crecen en nidos celulares separados por estroma fibroso desmoplásico, y que con frecuencia producen mucina. Desmoplasico:
- Los tumores infiltrativos son la forma mas comun, causa engrosamiento e induracion de la pared de la vesicula o de los ductos, se pueden extender y envolver. Estos tumores se expanden al plano subseroso. El tumor se disemina en la cavidad peritoneal, que puede ocurrir a traves del plano subseroso. Los nodulas o formadores de masa, muestran una temprana invasion a traves de la pared de la vesicula al higado o estrucutras vecinas. A pesar de esto, es mejor tratar por medios quirurgicos las formas nodulares que las infiltrativas donde los margenes no estan definidos. Los papilares se exhiben como polipoides o aspecto de coliflor y llenan la luz de la vesicula con pequeña invasion a la pare. El pronostico de esta forma es el mejor.
- El CCA intra-hepático se confunde a menudo con los adenocarcinomas metastásicos. Deben descartarse el carcinoma de vesícula biliar, la estenosis benigna y el síndrome de Mirizzi.
- Menor dilatación periferica de los conductos biliares Extrahepatico: dilatacion significante de los conductos.
- Los CCA intrahepáticos se confunden con con cánceres que surgen del hígado (CHC). Solamente 1 de cada 10 cánceres de conductos biliares es intrahepático. Los tumores de Klatskin son los tumores más comunes de los cánceres de los conductos biliares, representan más de las mitad de los casos, estan agurpados dentro de los extrahepáticos. Los distales tienen frecuencia de 2-3 por cada 10 cánceres de conductos biliares.
- Esta clasificacion sirve para los colangiocarcinomas perihiliares (klatskin) según el compromiso de 1 o ambos conductos hepaticos…
- Entre los más raros se encuentran: tipo carcinoide, carcinoma de células pequeñas, melanomas malignos, linfomas y sarcomas.
- presentacion inicial con una lesion palbable en el higado. Cuando los sintomas ocurren estos pueden incluir dolor no especifico en el cuadrante superior derecho. La ictericia ocurre de manera tardia
- PSC: colangitis esclerosante primaria Los marcadores tumorales pueden estar elevados pero ninguno de ellos es específico y pueden elevarse con otras malignidades gastroenterológicas y ginecológicas, al igual al comienzo de un proceso inflamatorio o infección del sistema biliar. CA: antígeno carbohidrato, antígeno sializado de Lewis En pacientes sin PSC la sensibilidad para CA 19-9 es de 53% con valores de 100 U/mL En pacientes con colangitis bacteriana o coledocolitiasis ocasionalmente pueden tener elevaciones significativas del CA 19-9
- DIA: digital image análisis
- http://www.cancer.org/acs/groups/cid/documents/webcontent/003084-pdf.pdf La estapa (estadio) de un tumor describe que tanto se ha expandido. Determinar el estadio del cancer es un factor importante para seleccionar opciones de tratamiento y estimar la sobrevivencia del paciente.
- Ejemplo
- Las nuevas técnicas y conocimiento quirúrgicos ha mejorado substancialmente desde el 2000 debido a la elección cuidadosa de los pacientes, esto ha disminuido las tasas de mortalidad quirúrgicas y aumentado las tasas de resección R0 (margen quirúrgico negativo).
- A, B, surgical technique for unilateral hepatojejunostomy with Roux-en-Y anastomosis and left hepatic lobectomy
- For resectable tumors, consider surgery. The choice of surgical approach will depend on the location of the tumor. For R0 resections, with negative surgical margins and lack of regional lymph node involvement, observation for recurrence, with imaging every 6 months for 3 years, or enrollment in a clinical trial of adjuvant systemic therapy should be considered. For resections with either positive margins (R1) or residual tumor or positive lymph nodes (R2), consider EBRT or systemic chemotherapy. For nonresectable or metastatic tumors, consider palliative biliary drainage if indicated, followed by intrabiliary PDT or brachytherapy, systemic chemotherapy with gemcitabine, or enrollment in a clinical trial evaluating new treatment modalities. Multimodality management based on liver transplantation might be appropriate for selected individuals with localized tumors and without any extrahepatic spread, but is available only at a few centers. Abbreviations: 5FU, 5-fluorouracil; EBRT, external beam radiation therapy; OLT, orthotopic liver transplant; PDT, photodynamic therapy; SBRT, stereotactic body radiotherapy.
- Los marcadores ayudan al diagnóstico pero no debemos confiar cien porciento en ellos porque los niveles pueden elevarse en condiciones inflamatorias y en otras malignidades gastrointestinales o ginecológicas. Alguna parte de la población no produce CEA.
- La sensibilidad y precisión de la USG para carcinoma de vesícula es de 85% y 80% respectivamente.
- Algoritmos del diagnóstico de carcinoma diagnosticado intra o postoperatorio