
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Measles
Similar to Measles (20)
Recently uploaded
Recently uploaded (20)
Measles
- 4. Measles (Rubeola) Dr . Anuradha Davey Associate Professor Community Medicine
- 5. Introduction • Measles means- Red Spots • It is Acute Viral exanthematous fever and leading cause of VPD • Most contagious disease known – And if ds is introduced in a virgin community- 90% of population will be affected – Immunity level needed to interrupt transmission is 94% or higher
- 6. • Prior to vaccination- epidemic after every 2-3 yrs • After vaccination- Interval increased to 5 years and peak of intensity decreased • Epidemic occur when susceptible population reached around 40%
- 7. Clinical features 3 stages • Prodromal • Eruptive phase • Post Eruptive phase
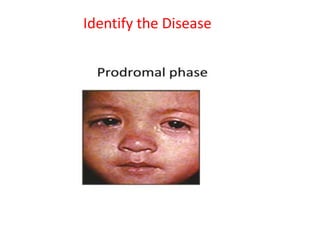
- 9. Prodromal: begins at 10 days after exposure and last for 4 days – Fever – Coryza – Sneezing – Nasal discharge – Cough – Redness of eyes – Lacrimation – Photophobia – May be vomiting or diarrhoea
- 10. • KOPLIK SPOT: 1-2 day before or after appearance of rash: small bluish-white spot on red base, smaller than head of a pin, against first and second lower molar tooth. “Pathognomic”
- 11. Koplik Spot
- 12. Eruptive phase: Rash appearance: after 4days of fever or 14 days of exposure – Dusky red, Maculo-papular rash ( pathognomic) – Discrete, confluent, blotchy – Begin behind the ear, in few hrs face and neck, down body in 2-3 days – Disappear in another 3-4 days in same order – Patient normally improves by 3rd day of rash and uncomplicated case recover within 7-10 days of onset of disease – Brownish discoloration lasting for 2 months or so During this phase, virus excrete from tear, nasal & throat secretion, urine, blood
- 14. Brownish discoloration of rash
- 15. Rash are because of circulating antibodies , result from interaction of T cells with virus infected cells in small blood vessels Patient with defective CMI- no rash
- 16. Post eruptive phase • Decreased immunity: chances of secondary infection • Loss of weight • Growth retardation • Diarrhoea • Cancrum oris • Pyogenic infection • Candidiasis • Reactivation of pulmonary TB
- 17. Complications • Measles associated diarrhoea • Pneumonia (most common cause of death) • Respiratory tract infection • Otitis media
- 18. Complications…Measles • Encephalitis (4-7 d after onset of rash) : 1: 1000 → 15% die • Sub acute sclerosing pan encephalitis: rare(1: 3,00,000) • develop many yrs after measles infection. • Diagnosis by CF AB in CSF. Fatal → severe personality changes, myoclonic seizures, motor impairment,coma and death over course of several months to years
- 20. Agent Category: Viral Disease-RNA paramyxovirus Only one serotype- so life long immunity • Easily destroyed by sunlight, acids and drying • BUT At sub zero temp: virus retain infectivity,
- 21. Agent….. • Source of Infection: Case or subclinical case No carrier stage Infective material: secretion from nose, throat, respiratory tract
- 22. • Direct- Person to person: droplet infection (the virus can survive for atlest two hours in fine droplets) • Indirect: droplet nuclei, articles freshly soiled with discharges Entry point : respiratory tract • Conjunctiva Transmission Communicability: prodromal phase and eruption of rashes. 4 days before and 4 days after the appearance of rash.
- 23. Host factor • Age: 6 mths to 3 year in developing countries and around 5 years in developed • Sex: equal in both sex but mortality following acute measles in greater in females at all age Immunity: If no previous immunity: all ages are susceptible •One attack gives life long immunity •Second attack is 90% •Immunity after vaccination is life lasting •Maternal ab persists from 6-9 mths after birth
- 24. Host continued……. • Increased risk of developing severe or fatal measles in the following cases: – Malnutrition (measles can precipitate kwashiorkor in borderline cases) – Vit A Deficiency – Severe immunological disorder such as advanced HIV Infection-
- 25. Environment • Tropical zone: dry season • Temperate zone: winter Overcrowding favours transmission Incubation period: From exposure to onset of fever: 10 days and From exposure to appearence of rash: 14 days •Overcrowding favours transmission Mini measles by passing the RT (through vaccination) : 7 days
- 26. • Measles infection during pregnancy→ spontaneous abortion, LBW, premature delivery • Atypical Measles Syndrome: high fever, pneumonia, pleural effusion, edema of hands & feet, hepatic abn, unusual rash ↓ seen in persons who received killed measles vaccine in the past & who were subsequently exposed to measles virus
- 27. Prevention and Control • Active Immunization- Primary method of prevention • Passive immunization- Administration of Immunoglobins • General measures
- 28. Diagnosis • History of contact with a case • C/F: maculopapular rash & koplik spots are pathognomic • Lab: A four fold rise in in measles antibody titre in acute or convalescent serum IgG antibodies appear shortly after rash,peak in 2 to 4 weeks and last for lifetime Viral particles can be demonstrated using RT- PCR
- 29. Active Immunization • Type of vaccine: Live attenuated vaccine- as freeze dried product (Chick embro or Human Diploid Cell line( Edmonston Zagreb strain vaccine) • Reconstitution: by cooled sterile diluents, must not be frozen • Sensitive to light : so kept in covered glass vials and reconstituted vaccine must be used in 6 hours
- 30. Continued…. • Dose: 0.5 ml, • Route: S/c or IM • Age: 9 months – THREE situation where vaccine can be given at 6 months if measles outbreak in India Malnourished child HIV (Asymptomatic ) infection and repeat dose at 6-9 mth with 4 weeks interval Contraindications: Pregnancy immunocompromised anaphylactic reaction to neomycin, gelatin or other components of vaccine
- 31. Immune response: humoral and cellular response with lower Ab titer Reaction: Mini measles illness 5-10 days after immunisation (15-20% of the vaccinees) Fever lasts for 1-2 days and rashes last for 3-4 days Immunity: develops after 11-12 days 99% protection when given at 12 month and 90% protection when given at 9 month because of slow sero conversion
- 32. Passive immunization • Normal human Immunoglobins • Dose: 0.25ml/kgbw • Within 6 days • Indication: vulnerable susceptible households contacts like immunocompromised children
- 33. General measures • Isolation : for one week from appearance of rash • Articles soiled with secretions or fluids from vesicles s/b incinerated or treated with disinfectants • Reporting of outbreaks to local health authorities
- 34. Treatment • No specific treatment • Supportive therapy- – Fever(antipyretics) – Dehydration (ORS) – Gen. Nutritional support – Antibiotic-for secondary bacterial infection – Vit A supplementation Dose: 2 doses 24 hours apart supplementaty doses: 6mth- 1 year: one lakh IU above 1 year: 2 lakh IU every 6 mthly
- 35. Definition of Elimination of Measles by WHO Absence of endemic measles for more than 12 months in the presence of adequate surveillance Indicator of measles Elimination: • Sustained measles incidence <1/100,000 population
- 36. Why Measles can be eliminated… • One sero type • Life long immunity • No chronic carrier state • No animal reservoir • Virus is easily destroyed
- 37. WHO Strategy for elimination Catch up Keep up Follow up • 1. Catch up: one time nation wide vaccination campaign targeting usually all children from 9mths to 14 yrs regardless of previous h/o vaccination or ds .
- 38. Continued…. 2. Keep up: Routine services aimed at vaccinating more than 95% of each successive birth cohort 3. Follow up: Subsequent nation wide vaccination campaign after every 2-4 years targeting all children born after catch up campaign First two are the supplementary vaccination campaign
- 39. Measles vaccination with HIV infection • Asymptomatic HIV infection: Measles is not a contraindication. – It is given at 6 months and additional dose at 9 months • Severely immuno-compromised: Measles contraindicated
- 40. •Thank you