
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Romantika (measles)
Similar to Romantika (measles) (20)
Recently uploaded
Recently uploaded (20)
Romantika (measles)
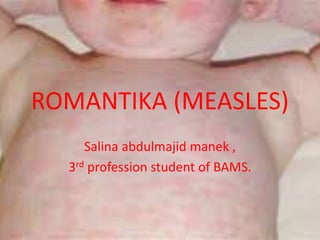
- 1. ROMANTIKA (MEASLES) Salina abdulmajid manek , 3rd profession student of BAMS.
- 2. INTRODUCTION • An acute highly infectious disease of childhood caused by a specific virus of the group myxoviruses. • It is clinically characterized by fever and cararrhal symptoms of upper respiratory tract (coryza, cough) followed by typical eash.
- 3. AGENT FACTORS • AGENT: Caused by RNA paramyxovirus. • SOURCE OF INFECTION: Is a case of measles. Carries are not known to occur. • INFECTIVE MATERIAL: Scretion of nose, throat and respiratory tract of case of measles during the prodromal period and the early stage of the rash. • COMMUNICABILITY: 4 days before and 5 days after the apperance of rash. • SECONDARY ATTACK RATE: Infection confres life long infectivity.
- 4. HOST FACTORS • AGE: B/W 6 month and 3 years of age and other childeren usually over 5 years. • SEX: both sexes • NIRITION: highly severe in malnourished child carring a mortality upto 400 times highly than in well nourished children. • ENVIRONMENTAL FACTORS: virus can spread in any season espicially a winter disease. • Epidemics occurs in winter • TXANOMISSION: Mainly by droplet nuclei from 4 days brfore the onset of rash until 5 days there after. • INCUBATION PERIOD: Commonly 10 days from exposure to onset of fever, and 14 days to appearance of rash.
- 5. ETIOPATHOGENESIS • Measles is caused by an RNA virus belongs to the paramyxovirus family. The virus transmitted by droplet spread from the secretion of the nose and throat usually 4 days befpre and 5 day after the rash. • The disease is highly contagious with secondary attack rates in susceptile household contact exceeding 90%.
- 6. The portal of entry is the respiratory tract where the virus multiples in the respiratory epithelium. Primary viremia occurs resulting in infection of the reticuloendothelial systemis followed by secondary viremia, which results is systemic symtoms.
- 7. PATHOGENESIS • After entering the body through repiratory tract by droplet infection, the virus quickly pass to the nearest lymp node multipy there and leak into the bloodstream, reaches R.E cells of liver, spleen and bone marrow, where they multipy and destroys cells and flow agai to blood stream in sufficient number as to affect many tissue in body mainly respiratory mucosa, alimentry mucosa, conjuctiva and skin. • The symptoms are mainly due to inflamatory reaction in these areas.
- 8. EPIDEMIOLOGy • Measles id endemic throughout the world. • In the past, epidemics tented to occurs irregularly. It is rarely subclinical. • Prior to the use of measles vaccine, the pek incidence was among childeen 5_10 yr of age. • The WHO estimate that over 40 million cases still occurs in worldwide contribution to 530000 deaths including 182000 in SEA region as reported in 2003.
- 9. • Now measles mortality has been reduced from 733000 in 2000 to 164000 in 2008 • In india measles is major cause of morbidity and a significant contribution to childhood mortality. • Propr to the immunization were record every third year. • With immunization coverage the interval etween cyclical peak incread and intensity minimized.
- 10. THREE STAGES 1.PRODROMAL/ CATARRHAL STAGE (FIRST 4 DAYS) 2.EXANTHEMATOUS STAGE (4TH TO 7TH DAY) 3.RECOVERS STAGE
- 11. 1. PREDROMAL • Beging 10 days after infection and lasts untill 14 days. • CHARACTEIZED: 1. Fever 2. Coryza 3. Sneezing 4. Nasal discharge 5. Cough 6. Redness of eye 7. Lacrimation 8. Often photophobia
- 12. • There may be vomiting or diarrhoea • On 2nd day-pathognomonic- kopliks spots apear in mucous membrane of mouth. • Tiny whitish or bluish white spot, against a reddish background, at level of upper 2nd molar teeth • Table salt crystal appear.
- 13. 2.) exanthematous (4th to 7th day) • High rise of temprature , face puffy, headaches, cough, photophobia, myalgia, lymph nodes may enlarge, spleen- may be palpable. • Rash – on 4th day, macilo papular flppear first, on forcehead and Behind the ears, at the downwards to whole of trunk and limbs upto palms and soles Initially- discrete, pink, blanch on pressure later confluent.
- 14. 3.) RECOVERY STAGE • Rapid, rashes fade away, leaving brownish discoloration of skine and areas of desquamation.
- 15. COMPLICATIONS Laryngitis bronchitis, broncho, pneumonia, conjuctivitis, otitismedia, albuminuria Neurological co plication include febrile convulsion. • In some cases vision loss has resulted in children infected with the measles virus as it has caused damage to the cornea (the clear front part of the eye) which becomes hazy and discolored in appearance. • Known as measles keratitis, infected children may tear excessively and need to avoid light due to extreme sensitivity. It is also noted that children who have poor diets and are deficient in vitamin A are at greater risk for more severe eye complications of measles. The measles virus can also affect the back of the eye especially the retina, which is the light-sensing part of the eye. “Measles virus can cause inflammation of almost any part of the back of the eye including the retina, blood vessels and optic nerve. Patients may lose vision due to swelling or scarring of the retina,”
- 16. MANAGEMENT • Isolation in well ventilated room • Concurrent disinfection of nasal and throat secretion • Light and clean clothes • Antipyretics to control fever • Plety of water and fruit juice because of loss of appetite • Correction of malnutrition with high quality diet
- 17. • Prophylactic antibiotic can be given • Attendants to use mask and gown • Watch for complication • Vitamin A for measles case management Vitamin A supprmentation is required in all cases of severe measles, a high dose of vitamin A ia give after diagnosis and reapeated next daty. AGE DAY1 follwing day 0-6 months- 50000IU -50000IU 6-11 months- 100000I -100000IU ≥12 months- 200000IU -200000IU
- 18. • MEASLES AND CHICKEN POX: • In case of double infection the 1st infection may diminish the severity of rash of the 2nd infection. • PRVENTION OF MEASLES: Achieving an immunization rate over 95% on going immunization against measles through successive generation of childeren.
- 19. • MEASLES VACCINATIONS • VACCINE: Tissue cultured vaccine either chick embryo or human diploid cell line. • AGE: 9 months • ADMINISTRATION: subcutaneous does of 0.5ml • REACTIONS: fvere • IMMUNITY: develops 11-12 days after vaccination • CONTRAINDICATION: pregnancy. • ADVERSE EFFECT OF VACCINE- Toxic shock syndrome (TSS) occurs when measles vaccine is contaminated or the same vial is used for more than 1 session the same day or the next day.
- 20. • Routine vaccination: • Minimum age: 9 months or 270 completed days. • Administer the primary dose of MMR vaccine at age 9 to 12 months, the second dose at age 15 through 18 months, and final (the 3rd) dose at age 4 through 6 years. • The 2nd dose must follow in 2nd year of life. However, it is given at anytime 4-8 weeks after the first dose • There is no need to give a stand-alone measles vaccine. •
- 21. • COMBIEND VACCINES: can be combiend with mumps rubella (MMR) or MMRV varicella or MR • IMMUNOGLOBINS: dose is 0.25 ml/body weight early in the incubation period. Should be given 3-4 days of exposure. • ERADICATION OF MEASLES: immunization by only 1 dose has been developed which is more heat stable • CONTROL MEASURES: • ISOLATION:for 7 day after the onset of rash, immunization of contact with I 2day of exposure. • IMMUNIZATON: at the beginning of an epidemic is essential to limitrd the spread.