Downloaded 87 times
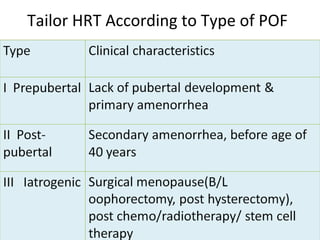
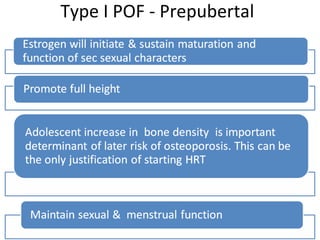
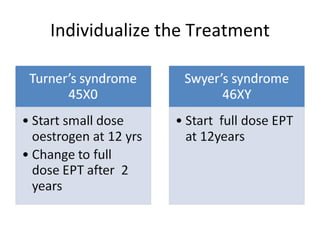
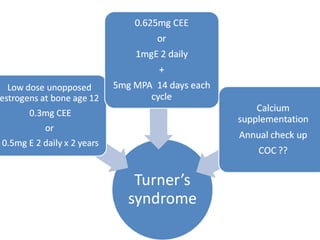
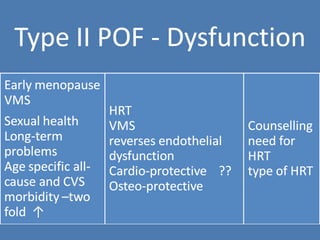
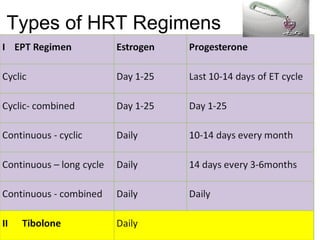
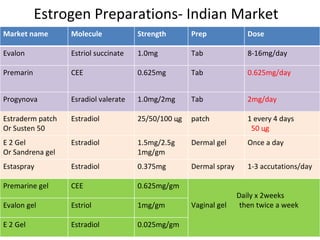
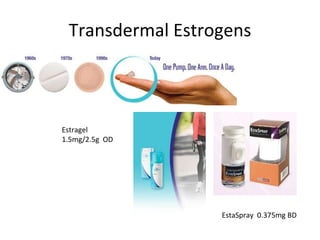
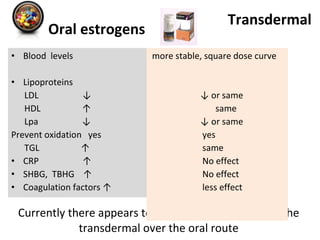
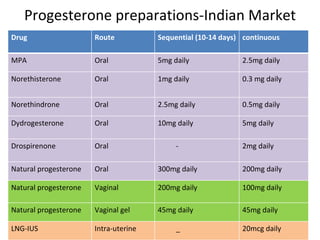


Hormone replacement therapy (HRT) is the recommended treatment for premature ovarian failure (POF) to replace the hormones lost due to the condition. HRT should be started at diagnosis and continued until natural menopause age to mimic the natural hormone levels. Full dose long-term HRT has not shown long-term ill effects unlike extended therapy that increases estrogen years. The type of HRT should be tailored to the type of POF, whether prepubertal, spontaneous ovulation may resume for some, or iatrogenic from sudden hormone drop requiring early high dose HRT. Options include oral and transdermal estrogen preparations with progestin.