Downloaded 74 times

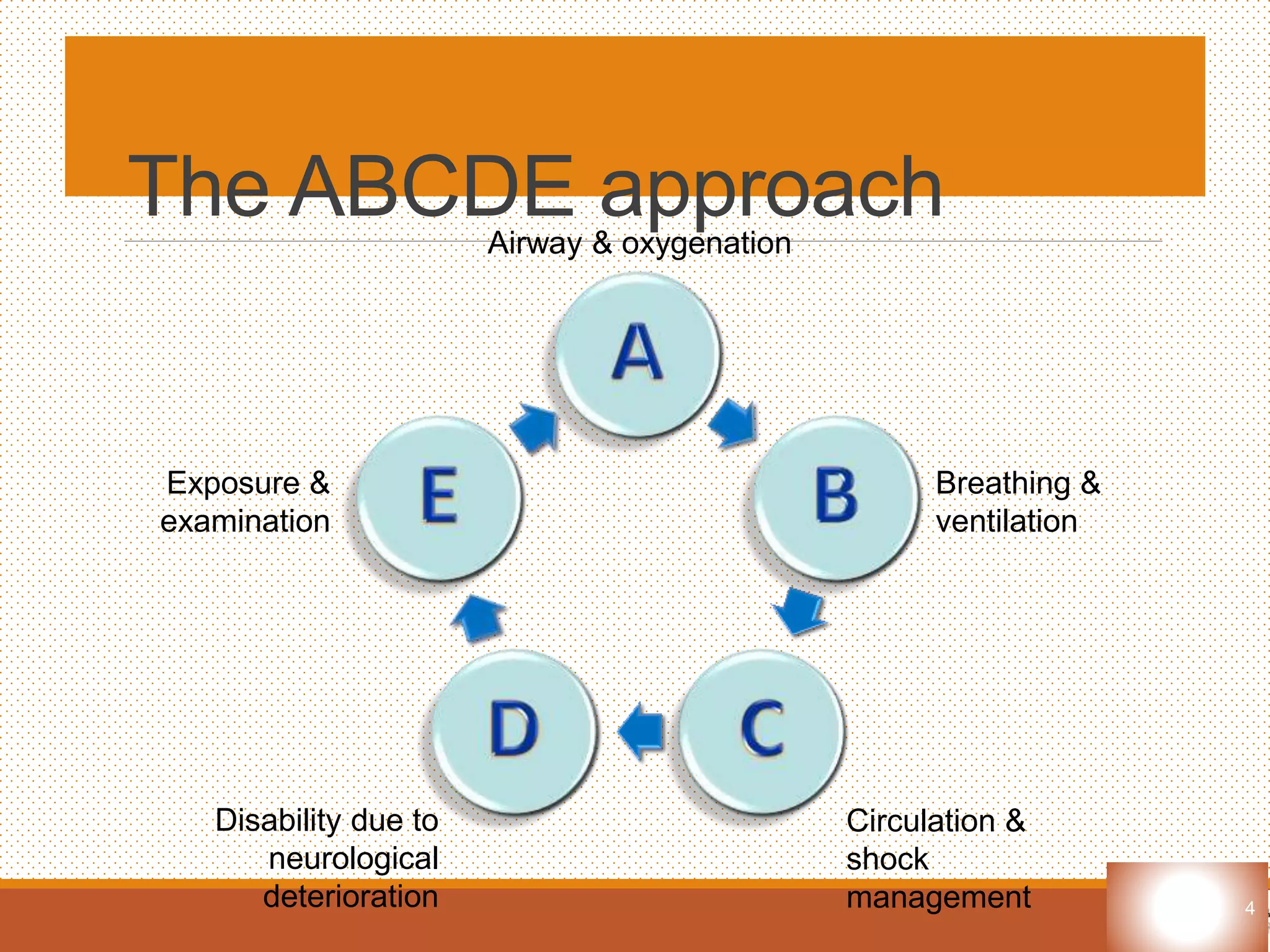
















The document outlines the ABCDE approach for assessing and treating critically ill patients, focusing on airway, breathing, circulation, disability, and exposure. It emphasizes the importance of rapid assessment, immediate life-saving interventions, and continuous reassessment. Additionally, it discusses the primary and secondary survey processes, detailing specific interventions for various life-threatening conditions.



































































