
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Diagnosis and Management of Endodontic-Periodontic Lesions
Similar to Diagnosis and Management of Endodontic-Periodontic Lesions (20)
Recently uploaded
Recently uploaded (20)
Diagnosis and Management of Endodontic-Periodontic Lesions
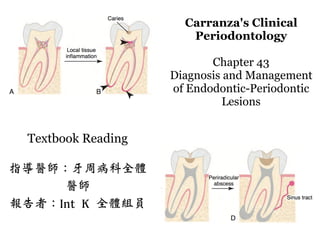
- 1. Carranza's Clinical Periodontology Chapter 43 Diagnosis and Management of Endodontic-Periodontic Lesions Textbook Reading 指導醫師:牙周病科全體 醫師 報告者:Int K 全體組員
- 2. Retrograde periodontitis • Advanced pulpitis - > pulp necrosis -> bone resorption at root apex or apical abscess • Periodontal tissue breakdown from apical to cervical
- 3. Orthograde periodontitis • Results from a sulcular infection.
- 4. Classification of endodontic- periodontic lesions. A, Primary pulpal infection can lead to chronic periradicular periodontitis B, Primary periodontal infection can lead to extensive breakdown of alveolar crest bone that migrates from the cervical area to the apex. C, Both primary pulpal and primary periodontal infection occur simultaneously D, Primary pulpal and primary periodontal infections can occur extensively in this “combined” endodontic-periodontic lesion.
- 5. Summary • Retrograde periodontitis • Orthograde periodontitis
- 6. Accessory canals • 59.5% of maxillary second premolars possess lateral canals • 78.2% of maxillary second premolars located in the apical regions of the root canals. • Located in midroot and cervical regions, frequencies at 16.2% and 4.0%, respectively. • 28.4% of permanent molars posses accessory canals in furcation regions
- 7. Accessory canals • Kirkham 100 permanent human teeth extracted as result of severe periodontal disease • 2 teeth possessed accessory canals within periodontal pockets
- 8. Lateral canal-led periodontal defect A, Bone loss is present in the furcation with sinus tract present on the buccal mucosa. Tooth #30 tested nonvital. B, During condensation, a large amount of sealer was expressed through a large lateral canal in the distal root.
- 9. Dentinal tubules • Tapered structure along the length from pulpodentinal complex (PDC) to the dentinoenamel junction (DEJ) • Diameter of 2.5 µm at PDC and 0.9 µm at the DEJ. • Permeability changes at different locations along the root surface • Bacterial colonization in tubules from infected root canals and periodontal pocket both demonstrated • Root planing shown to decrease dentin permeability
- 10. Iatrogenic defects • iatrogenic defects such as vertical root fractures and tooth p forations.
- 11. Summary • Retrograde Periodontitis • Orthograde Periodontitis • Accessory canals • Dentinal tubules • Iatrogenic defects
- 12. Factors Initiating Pulpal Diseases • Microorganisms • Trauma • Excessive heat • Restorative procedures • Restorative agents • Malocclusion.
- 13. Classification of Pulpal and Apical Diseases American Association of Endodontists revised terminology published in 2009 in volume 35 of the Journal of Endodontics (page 1634)
- 14. Biologic Effects of Pulpal Infection on Periodontal Tissues • Biofilm is composed of 15% cellular and 85% matrix • Proteolytic bacteria predominate in early root canal infections • Viruses play in the pathogenesis of both periodontal and endodontic disease • Gingival herpes viruses associated with the increased growth of pathogenic periodontal bacteria 22,45 • Epithelial rests, cholesterol crystals, Russell bodies, Rushton hyaline bodies, and Charcot-Leyden crystals.125 • Responsible for the lack of healing of apical lesions in teeth that have received appropriate endodontic treatment.125 22. Contreras A, Slots J: Typing of herpes simplex virus from human periodontium. Oral Microbiol Immunol 16:63–64, 2001. 45. Glick M, Trope M, Pliskin ME: Detection of HIV in the dental pulp of a patient with AIDS. J Am Dent Assoc 119:649–650, 1989. 125. Rothstein I, Simon JH: The endo-perio lesion: a critical appraisal of the disease condition. Endod Topics 13:34–56, 2006.
- 15. Cellulitis • Dissect PDL space and result in the formation of a deep but narrow periodontal pocket. • Whether the probing defect is the result of an endodontic or periodontal problem.
- 16. continued tooth mobility, and occlusal trauma splinting is sometimes necessary to help stabilize the tooth and allow for potential repair of the apical tissues
- 17. Summary • Factors Initiating Pulpal Diseases • Classification of Endodontic Disease • Biologic Effects of Pulpal Infection - > Periodontal Tissues