
Recommended
Recommended
More Related Content
Similar to By Beth Han, Wilson M. Compton, Carlos Blanco, and Lisa J. Col
Similar to By Beth Han, Wilson M. Compton, Carlos Blanco, and Lisa J. Col (20)
More from TawnaDelatorrejs
More from TawnaDelatorrejs (20)
Recently uploaded
Recently uploaded (20)
By Beth Han, Wilson M. Compton, Carlos Blanco, and Lisa J. Col
- 1. By Beth Han, Wilson M. Compton, Carlos Blanco, and Lisa J. Colpe Prevalence, Treatment, And Unmet Treatment Needs Of US Adults With Mental Health And Substance Use Disorders ABSTRACT We examined prevalence, treatment patterns, trends, and correlates of mental health and substance use treatments among adults with co-occurring disorders. Our data were from the 325,800 adults who participated in the National Survey on Drug Use and Health in the period 2008–14. Approximately 3.3 percent of the US adult population, or 7.7 million adults, had co-occurring disorders during the twelve months before the survey interview. Among them, 52.5 percent received neither mental health care nor substance use treatment in the prior year. The 9.1 percent who received both types of care tended to have more serious psychiatric problems and physical comorbidities and to be involved with the criminal justice system. Rates of receiving care only for mental health, receiving treatment only for substance use, and receiving both
- 2. types of care among adults with co-occurring disorders remained unchanged during the study period. Low perceived need and barriers to care access for both disorders likely contribute to low treatment rates of co-occurring disorders. Future studies are needed to improve treatment rates among this population. S ubstance use disorders and mental disorders influence each other, and their combined presentation (here- after referred to as co-occurring disorders) results in more profound functional impairment; worse treatment out- comes; higher morbidity and mortality; in- creased treatment costs; and higher risk for homelessness, incarceration, and suicide than each of the individual disorders.1–4 Current treat- ment guidelines recommend that people with co- occurring disorders receive treatments for both disorders.5–7 However, little is known about the twelve-month prevalence, service use patterns, correlates of mental health and substance use treatments, and unmet treatment need among US adults with co-occurring disorders. Recent studies indicate that the prevalence of opioid use disorders and marijuana use among adults has increased in recent years.8,9 It is im- portant to determine whether these specific in- creases led to greater overall prevalence of co-
- 3. occurring disorders, because adults with opioid or marijuana use disorders are likely to have co- occurring mental illness.8,9 Also, two recent stud- ies reported that between 2005–07 and 2014 and between 2004 and 2013, respectively, among the overall US adult population, receipt of mental health care increased (primarily as a result of increasing use of psychiatric medications), and receipt of substance use treatment remained stable.10,11 However, it is unknown whether there have been similar changes in patterns of care for adults with co-occurring disorders. The Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act of 2008 required insurance coverage of mental health and substance use treatments to be equal to cov- erage of general medical care.12 Moreover, pro- visions of the Affordable Care Act (ACA) may doi: 10.1377/hlthaff.2017.0584 HEALTH AFFAIRS 36, NO. 10 (2017): 1739–1747 ©2017 Project HOPE— The People-to-People Health Foundation, Inc. Beth Han is a researcher at the Substance Abuse and Mental Health Services Administration, in Rockville, Maryland. Wilson M. Compton ([email protected]) is deputy director of the
- 4. National Institute on Drug Abuse, in Rockville. Carlos Blanco is director of the Division of Epidemiology, Services, and Prevention Research, National Institute on Drug Abuse. Lisa J. Colpe is chief of the Office of Clinical and Population Epidemiology Research, National Institute of Mental Health, in Bethesda, Maryland. October 2017 36:10 Health Affairs 1739 Behavioral Health Care o n O cto b e r 1 1 , 2 0 1 7
- 6. a ffa irs.o rg / D o w n lo a d e d fro m http://content.healthaffairs.org/ facilitate access to and integration of mental health care and substance use treatment for adults with co-occurring disorders.13–17 The ACA expanded and highlighted parity of insurance coverage of treatments for mental illness and substance use disorders. It also emphasized expanding coverage and improving quality
- 7. through better integration of behavioral with general medical services.14–17 It is unknown whether these policies have led to changes in treatment rates of co-occurring disorders. Thus, using a large, nationally representative data set on co-occurring disorders and mental health and substance use treatments, we exam- ined the following understudied questions:What was the recent prevalence of twelve-month co- occurring disorders among adults in the United States? What were the patterns of mental health and substance use treatments received by adults with co-occurring disorders? Did these patterns change during the period 2008–14? What rea- sons for not receiving mental health and sub- stance use treatments were reported by adults with co-occurring disorders who perceived un- met treatment needs? Addressing the gaps in knowledge inherent in our research questions may identify where specialized services or targeted outreach efforts might be developed and may improve treatment rates for both disorders among this population. Study Data And Methods Data Sources We examined data on adults ages eighteen and older who participated in the Na- tional Survey on Drug Use and Health in the period 2008–14. We used that study period be- cause data on mental illness are available start- ing with 2008 and because data on substance use disorders after 2015 are not comparable with previous data, because of changes in the survey items.
- 8. The National Survey on Drug Use and Health was conducted each year by the Substance Abuse and Mental Health Services Administration (SAMHSA). It provides nationally representative data on mental illness, mental health care, sub- stance use disorders, and substance use treat- ment among the US civilian noninstitutional- ized population ages eighteen and older. We calculated an annual mean weighted response rate of 63.5 percent for the 2008–14 surveys, according to the definition of response rate 2 of the American Association for Public Opinion Research.19 Details regarding survey methods have been published elsewhere.18 Measures ▸ MENTAL ILLNESS: Mental illness among adults ages eighteen and older was defined as currently having or at any time in the past year having had a diagnosable mental disorder (ex- cluding developmental disorders and substance use disorders) of sufficient duration to meet the diagnostic criteria specified in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edi- tion (DSM-IV).20 Based on data from the 2008–12 Mental Health Surveillance Study, a model was devel- oped to predict both past-year mental illness sta- tus (yes or no) and serious mental illness status (yes or no) for each respondent in the adult samples of the National Survey on Drug Use and Health since 2008.21 We used the mental
- 9. illness variable to identify respondents with mental disorders, and we used the serious men- tal illness variable to control for the severity of mental illness in multivariable models. ▸ SUBSTANCE USE DISORDERS: The surveys estimated substance use disorders (dependence on or abuse of alcohol or an illicit drug) during the previous twelve months based on assess- ments of individual diagnostic criteria in the DSM-IV.20 The severity of substance use disor- ders was measured by the number of criteria met across these substances.22–25 ▸ MENTAL HEALTH CARE AND PERCEIVED UN- MET NEED: All adult survey respondents were asked to report on their receipt of inpatient or outpatient care or receipt of prescription medi- cations for mental health problems in the past year. Inpatient care includes services received at the following locations: a psychiatric hospital, the psychiatric unit of a general hospital, the medical unit of a general hospital for mental health treatment, or another type of hospital for mental health care. Outpatient care includes services received at following locations: a com- munity mental health center, the office of a pri- vate therapist for mental health care (a psychol- ogist, psychiatrist, social worker, or counselor), the office of a private physician (nonpsychia- trist), an outpatient medical clinic for mental health care, a day treatment program for mental health care, or another type of facility for mental health care. The surveys asked all adult respondents
- 10. whether they perceived that they had had unmet need for mental health care in the past year. Those who perceived this need for care and did not receive it were asked to report reasons why they did not receive it. ▸ SUBSTANCE USE TREATMENT AND PER- CEIVED UNMET NEED: Substance use treatment refers to treatment received for the use of illicit drugs or alcohol or for medical problems associ- ated with that use.26 It includes treatment re- ceived in the past year at a hospital (inpatient), rehabilitation facility (outpatient or inpatient), Behavioral Health Care 1740 Health Affairs October 2017 36:10 o n O cto b e r 1 1 , 2 0 1 7 b
- 12. irs.o rg / D o w n lo a d e d fro m http://content.healthaffairs.org/ mental health center, emergency department (ED), the office of a private physician, or prison or jail. The surveys asked adults with substance use problems whether they perceived that they had had unmet need for substance use treatment in the past year. Those who perceived unmet need for that treatment and who had not received it were asked to report reasons why they did not receive it. ▸ HEALTH STATUS: The surveys captured
- 13. respondents’ self-rated health and the number of ED visits in the past year. Physical co- morbidities were assessed by asking adult respondents if they had been told by a doctor or other health care professional in the past year that they had hypertension, heart disease, diabe- tes, stroke, asthma, bronchitis, sinusitis, pneu- monia, hepatitis, sexually transmitted diseases, HIV/AIDS, ulcers, tuberculosis, sleep apnea, tin- nitus, pancreatitis, cirrhosis, or lung cancer.We used this list to compute the total number of physical comorbidities. ▸ SOCIODEMOGRAPHIC CHARACTERISTICS AND CRIMINAL JUSTICE INVOLVEMENT: We ana- lyzed respondents’ age, sex, race/ethnicity, edu- cation, employment status, health insurance sta- tus, marital status, annual family income as a percentage of the federal poverty level, residence in any Metropolitan Statistical Area, census re- gion, and survey year. We also assessed justice involvement, which was defined by having had any arrest and booking, probation, or parole in the past year.27 Item response rates on the surveys are high. Moreover, missing values are imputed in the survey using predictive mean neighborhoods28,29 or a modified version of that method.29 Statistical Analyses Analyses were con- ducted in four stages. First, we estimated the twelve-month prevalence of co-occurring disor- ders among US adults, the twelve-month preva-
- 14. lence of receiving mental health care and sub- stance use treatment, and detailed treatment patterns among adults with co-occurring disor- ders. Second, we assessed the twelve-month prevalenceof receipt of neithertype of care, men- tal health care only, substance use treatment only, and both types of care among this popula- tion, according to sociodemographic character- istics, health status, serious mental illness, se- verity of substance use disorders, and criminal justice involvement. Third, we used bivariable and multivariable multinomial logistic regression models to assess correlates of receipt of mental health and sub- stance use treatments. Multicollinearity (using variance inflation factors) and potential interac- tion effects between examined factors were as- sessed and were not found in the final multivari- able model. Finally, we assessed the prevalence of per- ceived unmet treatment needs for mental health care and for substance use treatment among adults with co-occurring disorders who did not receive the corresponding care and who pre- sented their commonly reported reasons for not receiving the care.We used SUDAAN, version 11.0.1,30 to account for the complex sample de- sign and sampling weights of the survey data. Limitations This study had several limita- tions. First, the surveys did not cover homeless people not living in shelters, active-duty mem- bers of the military, or people residing in insti-
- 15. tutions. However, the surveys covered homeless people who lived in shelters and included adults who had been discharged from institutions at the time of the survey interview. Second, the surveys did not measure the qual- ity and exact timing of receipt of mental health care and substance use treatment at different settings. Third, the surveys did not ask about substance use treatment provided in outpatient medical clinics. Fourth, the surveys did not measure the fre- quency or duration of substance use treatment. Fifth, they did not query for specific mental dis- orders, except for major depressive episode and substance use disorders. However, mood disor- ders, anxiety disorder, eating disorder, adjust- ment disorder, and psychotic symptoms (delu- sions, hallucinations, or both) are likely to be represented among adults with mental illness in the sample.31 Finally, the survey data were self-reported and subject to recall bias. Study Results Based on the 325,800 sampled adults ages eigh- teen and older from the 2008–14 surveys, we estimated that an annual average of 3.3 percent of the US adult population, or 7.7 million adults, Our findings document a large gap between the prevalence of co-
- 16. occurring disorders and treatment rates. October 2017 36:10 Health Affairs 1741 o n O cto b e r 1 1 , 2 0 1 7 b y H W T e a m H e a lth A
- 18. d e d fro m http://content.healthaffairs.org/ had co-occurring mental illness and substance use disorders in the past year (data not shown). In particular, among the 42.1 million adults with mental illness, 18.2 percent also had substance use disorders. Among the 20.3 million adults with substance use disorders (annual average), 37.9 percent also had mental illness. The overall prevalence of co-occurring disorders was gener- ally stable during the study period (for the over- all trend, p = 0.7785). Patterns Of Mental Health And Substance Use Treatments Among adults with co-occur- ring disorders, 43.6 percent received any mental health care in the prior year (Exhibit 1), which was slightly higher than the corresponding mental health treatment rate among adults with mental illness, regardless of co-occurring status (42.1 percent; data not shown). Also among adults with co-occurring disorders, 13.0 percent received substance use treatment in the past year (Exhibit 1), which was 67 percent higher than the corresponding substance use treatment rate among adults with substance use disorders re-
- 19. gardless of co-occurring status (7.8 percent; data not shown). Among adults with co-occurring disorders, 9.1 percent received both mental health care and substance use treatment, 34.5 percent received mental health care only, 3.9 percent received substance use treatment only, and 52.5 percent received neither mental health care nor substance use treatment (Exhibit 1). For de- tailed patterns of receiving outpatient and in- patient mental health care and substance use treatment, see the online Appendix Exhibit.32 Twelve-Month Prevalence Of Treatments Exhibit 2 shows that among US adults with co- occurring disorders, the annual rates of receiv- ing neither type of care, mental health care only, substance use treatment only, and both types of care remained stable during the study period. Correlates Of Treatments Consistent with the bivariable results, our multivariable results showed that the adjusted prevalence of receiving neither type of care, mental health care only, substance use treatment only, and both types of care remained stable during the study period (Exhibit 3). Compared to receiving both types of care, after adjustment for covariates, the following charac- Exhibit 1 Mental health and substance use treatment received in the prior year by US adults with
- 20. co-occurring disorders, 2008–14 Treatment received in the prior year Annual average weighted percentage Any mental health or substance use treatment 47.5 Any mental health treatment 43.6 Any outpatient treatment 24.1 Any inpatient treatment 5.5 Any prescription medication for mental health problems 37.2 Any substance use treatment 13.0 Both mental health and substance use treatment 9.1 Mental health only 34.5 Substance use only 3.9 Neither mental health nor substance use treatment 52.5 SOURCE Authors’ analysis of data for 2008–14 from the National Survey on Drug Use and Health. NOTES N = 15,800. The Substance Abuse and Mental Health Services Administration requires that any description of overall sample sizes based on the restricted- use data files be rounded to the nearest 100 to minimize potential disclosure risk. “Any mental health care” is inpatient or outpatient mental health care or prescription medication for mental health problems (for a fuller definition, see the text). Exhibit 2
- 21. Mental health and substance use treatment received in the prior year by US adults with co-occurring disorders, 2008–14 Adults who received: Versus receiving both types of care, odds ratio of receiving: Year Neither Mental health only Substance use only Both Neither Mental health only Substance use only 2008 (ref) 54.0% 33.1% 4.1% 8.9% 1.0 1.0 1.0 2009 51.3 35.5 3.9 9.3 0.9 1.0 0.9 2010 51.1 35.8 3.1 10.0 0.8 1.0 0.7 2011 53.2 33.7 4.0 9.2 0.9 1.0 0.9 2012 53.1 33.0 4.9 9.0 1.0 1.0 1.2 2013 51.7 36.9 3.3 8.0 1.1 1.2 0.9 2014 53.3 33.4 3.9 9.5 0.9 0.9 0.9 SOURCE Authors’ analysis of data for 2008–14 from the
- 22. National Survey on Drug Use and Health. NOTES N = 15,800. The Substance Abuse and Mental Health Services Administration requires that any description of overall sample sizes based on the restricted- use data files has to be rounded to the nearest 100 to minimize potential disclosure risk. Percentages might not sum to 100 because of rounding. The odds ratios were calculated from bivariable multinomial logistic regressions. None of the differences between the reference year and other years was significant (p < 0:05). None of the unadjusted odds ratios was significant. Behavioral Health Care 1742 Health Affairs October 2017 36:10 o n O cto b e r 1 1 , 2 0 1 7 b y H
- 24. irs.o rg / D o w n lo a d e d fro m http://content.healthaffairs.org/ teristics were associated with receiving neither type of care: having no physical comorbidities, having no serious mental illness, meeting three or fewer substance use disorder criteria across substances, having no criminal justice involve- ment, and being uninsured. Similarly, the fol- lowing characteristics were associated with re- ceiving mental health care only: meeting three or fewer substance use disorder criteria across sub- stances and having no criminal justice involve- ment. And the following characteristics were as- sociated with receiving substance use treatment
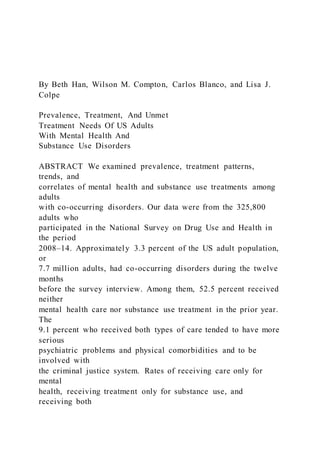
- 25. only: having no physical comorbidities, having no serious mental illness, having criminal justice involvement, and being uninsured. Perceived Unmet Need For Mental Health Care Among the 7.7 million US adults with co- occurring disorders, 4.3 million (56.4 percent) did not receive mental health care in the past year. Among those who did not receive care, 1.1 million (24.3 percent) perceived an unmet need for it in the past year (data not shown) and reported their reasons. The most common were inability to afford the treatment cost (52.2 percent), not knowing where to go for treatment (23.8 percent), and believing at the time that the problem could be handled without treatment (23.0 percent) (Exhibit 4). Perceived Unmet Need For Substance Use Treatment Among the 7.7 million US adults with co-occurring disorders, 6.1 million (87.0 percent) did not receive substance use treatment in the past year. Among those who did not receive treatment, only 633,000 (9.5 per- cent) perceived an unmet need for it in the past year (data not shown) and reported their rea- sons. The most common was not being ready to stop using the substance(s) (38.4 percent), and the second most common was having no health insurance and being unable to afford the cost (35.1 percent) (Exhibit 5). Discussion Using recent nationally representative data, we examined the annual prevalence, treatment pat- terns, correlates, and unmet treatment needs
- 26. for co-occurring disorders among adults in the United States. Approximately 3.3 percent of the US adult population (or 7.7 million adults) had twelve-month co-occurring disorders (annual averages). In contrast to our earlier findings on the increases in opioid use disorders and marijuana use,8,9 the prevalence of alcohol use disorders among US adults declined33—which may help explain why the prevalence of co-occur- ring disorders was stable during the period 2008–14. Despite current treatment guidelines that call for both types of disorders to be treated when they co-occur,5–7 only 9.1 percent of adults with co-occurring disorders received both types of care in the past year, and 52.5 percent received neither mental health care nor substance use treatment. Our findings document a large gap between the prevalence of co-occurring disor- ders and treatment rates among adults with those disorders in the United States. Compared to adults with mental illness, adults with co-occurring disorders had a slightly higher mental health treatment rate (43.6 percent ver- Exhibit 3 Treatment patterns among US adults with co-occurring disorders, by selected characteristics, 2008–14 Versus receiving both types of treatment, adjusted odds ratio of receiving:
- 27. Neither type of treatment Mental health treatment only Substance use treatment only Year 2008 (ref) 1.0 1.0 1.0 2009 1.0 1.1 0.9 2010 1.0 1.1 0.8 2011 1.2 1.1 1.1 2012 1.1 1.1 1.4 2013 1.2 1.3 1.0 2014 0.9 0.9 1.2 Number of physical comorbidities 0 (ref) 1.0 1.0 1.0 1 0.7* 1.1 0.5** 2 0.5*** 0.9 0.6 3 or more 0.9 1.0 0.9 Serious mental illness Yes 0.3**** 0.8* 0.4**** No (ref) 1.0 1.0 1.0 Number of substance use disorder criteriaa met 1–3 (ref) 1.0 1.0 1.0 4–6 0.4*** 0.4*** 1.1 7–9 0.1**** 0.2**** 0.9
- 28. 10 or more 0.1**** 0.1**** 0.9 Criminal justice involvementb in prior year Yes 0.3**** 0.4**** 1.5** No (ref) 1.0 1.0 1.0 Type of health insurance Private only (ref) 1.0 1.0 1.0 None 2.1**** 1.0 1.7** Medicaid 0.9 1.0 1.3 Other 1.0 0.9 1.3 SOURCE Authors’ analysis of data from the 2008–2014 National Survey on Drug Use and Health. NOTES N = 15,800. The Substance Abuse and Mental Health Services Administration requires that any description of overall sample sizes based on the restricted-use data files be rounded to the nearest 100 to minimize potential disclosure risk. Odds ratios were adjusted for all of the variables in Exhibit 3 and also controlled for age, sex, race/ethnicity, education, employment, marital status, family income as a percentage of the federal poverty level, census region, residence in any Metropolitan Statistical Area, self-rated health, and the number of emergency department visits in the past year. aCriteria for substance use disorder from American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders (Note 20 in text). bAny arrest and booking, probation, or parole. *p < 0:10 **p < 0:05 ***p < 0:01 ****p < 0:001 October 2017 36:10 Health Affairs 1743
- 29. o n O cto b e r 1 1 , 2 0 1 7 b y H W T e a m H e a lth A ffa irs b
- 31. m http://content.healthaffairs.org/ sus 42.1 percent). Compared to adults with sub- stance use disorders, adults with co-occurring disorders had a 67 percent higher substance use treatment rate (13.0 percent versus 7.8 per- cent). We found that adults with co-occurring disorders who received both types of care tended to have more serious psychiatric problems and physical comorbidities and to be more likely to be involved with the criminal justice system than those who did not receive both types of care. This suggests that appropriate services are reaching some of the people in most need. However, low perceived need (especially for treating substance use disorders) and barriers to care access for both disorders likely contribute to low treatment rates of co-occurring disorders. Low perceived need has consistently been a major barrier to treatment seeking.34 The Na- tional Comorbidity Survey Replication studies found that low perceived need was reported by 44.8 percent of respondents with a disorder who did not seek treatment34 and that 23.1–47.3 per- cent of people with lifetime substance use disor- ders never made treatment contact.35 We found that almost a quarter of adults with co-occurring disorders who did not receive mental health care perceived an unmet need for that care. Of those,
- 32. more than half reported an inability to afford the treatment cost, and almost another quarter did not know where to go for treatment—which sug- gests a need to improve the awareness of treat- ment locations. By contrast, among adults with co-occurring disorders who did not receive sub- stance use treatment, fewer than a tenth per- ceived an unmet need for substance use treat- ment. This indicates that increasing the perception of need for treatment may be even more critical in the case of substance use disor- ders to increase treatment rates.Without perceiv- ing need for treatments for both types of disor- ders, it is unlikely that these adults will seek or receive timely substance use treatment and men- tal health care. In addition to low perceived need among adults with co-occurring disorders, financial bar- riers can impede treatment seeking.13–15,36,37 Con- sistent with the results of these previous studies, we found that among adults with co-occurring disorders who perceived a need for mental health care but did not receive it, 52.2 percent reported that they could not afford the cost. Also among adults with co-occurring disorders who per- ceived a need for substance use treatment but did not receive it, 35.1 percent reported that they had no health insurance and could not afford the cost. Importantly, this study found that treatment rates of all types for adults with co-occurring disorders did not change significantly during the period 2008–14. Although barriers may be greater for substance use treatment than for
- 33. mental health care,11 for adults with co-occurring disorders, we did not find an increase in receipt of only mental health care, either. In contrast, other research has found that receipt of mental health treatment increased among the overall Exhibit 4 Percentages of adults with co-occurring disorders and a perceived unmet need for mental health care who reported common reasons for not receiving that care in the prior year SOURCE Authors’ analysis of data for 2008–14 from the National Survey on Drug Use and Health. NOTES N = 2,500. The Substance Abuse and Mental Health Services Administration requires that any description of overall sample sizes based on the restricted-use data files be rounded to the nearest 100 to minimize potential disclosure risk. The percentages were annual average weighted estimates. Exhibit 5 Percentages of adults with co-occurring disorders and a perceived unmet needs for substance use treatment who reported common reasons for not receiving that treatment in the past year Authors’ analysis of data for 2008–14 from the National Survey on Drug Use and Health. NOTES N = 600. The Substance Abuse and Mental Health Services Administration requires that any descrip- tion of overall sample sizes based on the restricted-use data files be rounded to the nearest 100 to
- 34. minimize potential disclosure risk. The percentages were annual average weighted estimates. Behavioral Health Care 1744 Health Affairs October 2017 36:10 o n O cto b e r 1 1 , 2 0 1 7 b y H W T e a m H e a
- 36. lo a d e d fro m http://content.healthaffairs.org/ adult population10,11,38 and among mentally ill baby boomers and Generation X38 during this time period, although substance use treatment in these groups remained unchanged.11 Also, we found that the interaction effect between survey year and health insurance status was not signifi- cant, which indicates that the impact of health insurance status on treatment outcomes among adults with co-occurring disorders did not vary by survey year. Thus, it appears that implementing the Mental Health Parity and Addiction Equity Act and the ACA created incentives for health care systems to address behavioral health issues14–16 that may have had an impact on overall mental health service delivery but might not yet have affected people with substance use disorders, including those with co-occurring disorders. Future re- search is needed to continue to assess trends in mental health care and substance use treat- ments among this population and examine
- 37. whether current incentives in the parity law and the ACA are insufficient, may need more time to have an impact, or may vary across states. The percentage of mental health facilities in the United States offering programs for patients with co-occurring disorders decreased from 58.4 percent in 2010 to 53.0 percent in 2014, although the percentage of substance use treat- ment facilities offering such programs increased from 37.2 percent in 2008 to 44.2 percent in 2014.39,40 We found that among adults with co- occurring disorders, 34.5 percent received men- tal health care only, and 3.9 percent received substance use treatment only. Thus, treatment rates of co-occurring disorders could be im- proved if patients entering treatment for mental disorders were screened for substance use disor- ders and given high-quality substance use treat- ment in mental health care settings. Specialty treatment programs for substance use problems do increasingly offer evaluation and treatment of co-occurring mental disorders. Adults who are referred to specialty substance use treatment may be more likely to receive treatment for co- occurring mental disorders. Future research is needed to understand why the percentage of US mental health facilities offering programs for patients with co-occurring disorders is declin- ing, and why fewer than half of US substance use treatment facilities offer programs for pa- tients with co-occurring disorders. Furthermore, we found that 52.5 percent of adults with co-occurring disorders received nei-
- 38. ther mental health care nor substance use treat- ment in the past year. Our results suggest a need to screen for and treat co-occurring disorders. Given the prevalence of these disorders, this ap- proach should be taken not just by specialty be- havioral health practitioners, but by clinicians throughout medicine.16 Efforts to integrate be- havioral health screening, referral, and treat- ment into general medical settings may benefit this vulnerable population. However, some pa- tients with co-occurring disorders have complex needs and may require specialty care. Conclusion This study provided recent national estimates on the twelve-month prevalence of co-occurring dis- orders among US adults, twelve-month patterns and correlates of mental health care and sub- stance use treatments, and unmet treatment needs among adults with co-occurring disorders in the United States. Despite current treatment guidelines, fewer than 10 percent of adults with co-occurring disorders receive treatment for both disorders, and fewer than 50 percent re- ceive treatment for just one disorder. Further- more, these treatment rates do not seem to have improved over time. Our study highlights the fact that low perceived need (especially for treat- ing substance use disorders) and barriers to care access for both disorders likely contribute to low treatment rates of co-occurring disorders. Our results suggest a need to screen for and treat these disorders. Future studies are needed to identify effective approaches to increasing treat- ment rates of co-occurring disorders among adults in the United States. ▪
- 39. More than half of adults with co- occurring disorders received neither mental health care nor substance use treatment in the past year. October 2017 36:10 Health Affairs 1745 o n O cto b e r 1 1 , 2 0 1 7 b y H W T e a m
- 41. o w n lo a d e d fro m http://content.healthaffairs.org/ Unrelated to the submitted work, Wilson Compton reports ownership of stock in General Electric Co., 3M Co., and Pfizer Inc. Carlos Blanco reports ownership of stock in General Electric Co. and Eli Lilly Inc. The findings and conclusions of this study are those of the authors and do not necessarily reflect the views of the Substance Abuse and Mental Health Services Administration, the National Institute on Drug Abuse of the National Institutes of Health, or the National Institute of Mental Health of the National Institutes of Health, within the US Department of Health and Human Services.
- 42. NOTES 1 Compton WM, Thomas YF, Stinson FS, Grant BF. Prevalence, correlates, disability, and comorbidity of DSM- IV drug abuse and dependence in the United States: results from the Na- tional Epidemiologic Survey on Al- cohol and Related Conditions. Arch Gen Psychiatry. 2007;64(5):566–76. 2 Mojtabai R, Chen LY, Kaufmann CN, Crum RM. Comparing barriers to mental health treatment and sub- stance use disorder treatment among individuals with comorbid major depression and substance use disorders. J Subst Abuse Treat. 2014; 46(2):268–73. 3 Grant BF, Stinson FS, Dawson DA, Chou SP, Dufour MC, Compton W, et al. Prevalence and co-occurrence of substance use disorders and in- dependent mood and anxiety disor- ders: results from the National Epi- demiologic Survey on Alcohol and Related Conditions. Arch Gen Psy- chiatry. 2004;61(8):807–16. 4 Hartz SM, Pato CN, Medeiros H, Cavazos-Rehg P, Sobell JL, Knowles JA, et al. Comorbidity of severe psy- chotic disorders with measures of substance use. JAMA Psychiatry.
- 43. 2014;71(3):248–54. 5 Watkins KE, Hunter SB, Burnam MA, Pincus HA, Nicholson G. Review of treatment recommendations for persons with a co-occurring affective or anxiety and substance use disor- der. Psychiatr Serv. 2005;56(8): 913–26. 6 Pettinati HM, O’Brien CP, Dundon WD. Current status of co-occurring mood and substance use disorders: a new therapeutic target. Am J Psy- chiatry. 2013;170(1):23–30. 7 Pettinati HM, Oslin DW, Kampman KM, Dundon WD, Xie H, Gallis TL, et al. A double-blind, placebo-con- trolled trial combining sertraline and naltrexone for treating co- occurring depression and alcohol dependence. Am J Psychiatry. 2010; 167(6):668–75. 8 Han B, Compton WM, Jones CM, Cai R. Nonmedical prescription opioid use and use disorders among adults aged 18 through 64 years in the United States, 2003–2013. JAMA. 2015;314(14):1468–78. 9 Compton WM, Han B, Jones CM, Blanco C, Hughes A. Marijuana use and use disorders in adults in the USA, 2002–14: analysis of annual
- 44. cross-sectional surveys. Lancet Psy- chiatry. 2016;3(10):954–64. 10 Creedon TB, Cook BL. Access to mental health care increased but not for substance use, while disparities remain. Health Aff (Millwood). 2016;35(6):1017–21. 11 Mark TL, Yee T, Levit KR, Camacho- Cook J, Cutler E, Carroll CD. Insur- ance financing increased for mental health conditions but not for sub- stance use disorders, 1986–2014. Health Aff (Millwood). 2016;35(6): 958–65. 12 Department of Labor [Internet]. Washington (DC): Department of Labor. News release, Administration issues final mental health and sub- stance use disorder parity rule; 2013 Nov 8 [cited 2017 Aug 10]. Available from: https://www.dol.gov/opa/ media/press/ebsa/EBSA20132158 .htm?keepThis=true&TB_iframe= true&height=600&width=850 13 Bishop TF, Press MJ, Keyhani S, Pincus HA. Acceptance of insurance by psychiatrists and the implications for access to mental health care. JAMA Psychiatry. 2014;71(2): 176–81. 14 Buck JA. The looming expansion and
- 45. transformation of public substance abuse treatment under the Afford- able Care Act. Health Aff (Millwood). 2011;30(8):1402–10. 15 Barry CL, Huskamp HA. Moving beyond parity—mental health and addiction care under the ACA. N Engl J Med. 2011;365(11):973–5. 16 Compton WM, Blanco C, Wargo EM. Integrating addiction services into general medicine. JAMA. 2015; 314(22):2401–2. 17 Olfson M, Kroenke K, Wang S, Blanco C. Trends in office-based mental health care provided by psy- chiatrists and primary care physi- cians. J Clin Psychiatry. 2014; 75(3):247–53. 18 Substance Abuse and Mental Health Services Administration. Population data/NSDUH [Internet]. Rockville (MD): SAMHSA; [last updated 2014 Sep 12; cited 2017 Sep 5]. Available from: http://www.samhsa.gov/data/ population-data-nsduh/reports 19 American Association for Public Opinion Research. Standard defini- tions: final dispositions of case codes and outcome rates for surveys. 8th edition. Oakbrook Terrace (IL): AAPOR; 2015. p. 52–53.
- 46. 20 American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. Washing- ton (DC): APA; 1994. 21 Center for Behavioral Health Statis- tics and Quality. National Survey on Drug Use and Health: alternative statistical models to predict mental illness [Internet]. Rockville (MD): Substance Abuse and Mental Health Services Administration; 2015 Sep [cited 2017 Aug 10]. Available from: https://www.samhsa.gov/data/ sites/default/files/NSDUH-N23-MI- Models-2015.pdf 22 Hasin DS, O’Brien CP, Auriacombe M, Borges G, Bucholz K, Budney A, et al. DSM-5 criteria for substance use disorders: recommendations and rationale. Am J Psychiatry. 2013; 170(8):834–51. 23 Beseler CL, Hasin DS. Cannabis di- mensionality: dependence, abuse, and consumption. Addict Behav. 2010;35(11):961–9. 24 Hasin DS, Liu X, Alderson D, Grant BF. DSM-IV alcohol dependence: a categorical or dimensional pheno- type? Psychol Med. 2006;36(12): 1695–705.
- 47. 25 Dawson DA, Saha TD, Grant BF. A multidimensional assessment of the validity and utility of alcohol use disorder severity as determined by item response theory models. Drug Alcohol Depend. 2010;107(1):31–8. 26 Han B, Hedden SL, Lipari R, Copello EAP, Kroutil LA. Receipt of services for behavioral health problems: re- sults from the 2014 National Survey on Drug Use and Health [Internet]. Rockville (MD): Substance Abuse and Mental Health Services Admin- istration; 2015 Sep [cited 2017 Aug 10]. Available from: https://www .samhsa.gov/data/sites/default/ files/NSDUH-DR-FRR3-2014/ NSDUH-DR-FRR3-2014/NSDUH- DR-FRR3-2014.htm 27 Saloner B, Bandara SN, McGinty EE, Barry CL. Justice-involved adults with substance use disorders: cov- erage increased but rates of treat- ment did not in 2014. Health Aff (Millwood). 2016;35(6):1058–66. 28 Rubin DB. Statistical matching using file concatenation with adjusted weights and multiple imputations. Journal of Business and Economic Statistics. 1986;4(1):87–94. 29 Center for Behavioral Health Statis-
- 48. tics and Quality. 2014 National Sur- vey on Drug Use and Health: meth- odological resource book, Section 10: editing and imputation report [Internet]. Rockville (MD): Sub- Behavioral Health Care 1746 Health Affairs October 2017 36:10 o n O cto b e r 1 1 , 2 0 1 7 b y H W T e a m H
- 50. n lo a d e d fro m http://content.healthaffairs.org/ stance Abuse and Mental Health Services Administration; 2016 Feb [cited 2017 Aug 10]. Available from: https://www.samhsa.gov/data/ sites/default/files/NSDUHmrb EditAndImp2014.pdf 30 Bieler GS, Brown GG, Williams RL, Brogan DJ. Estimating model- adjusted risks, risk differences, and risk ratios from complex survey data. Am J Epidemiol. 2010;171(5): 618–23. 31 Karg RS, Bose J, Batts KR, Forman- Hoffman VL, Liao D, Hirsch E, et al. Past year mental disorders among adults in the United States: results from the 2008–2012 Mental Health Surveillance Study [Internet]. Rock-
- 51. ville (MD): Substance Abuse and Mental Health Services Administra- tion; 2014 Oct [cited 2017 Aug 10]. Available from: https://www .samhsa.gov/data/sites/default/ files/NSDUH-DR-N2MentalDis- 2014-1/Web/NSDUH-DR-N2Mental Dis-2014.htm 32 To access the Appendix, click on the Details tab of the article online. 33 Hedden SL, Kennet J, Lipari R, Medley G, Tice P, Copello EAP, et al. Behavioral health trends in the United States: results from the 2014 National Survey on Drug Use and Health [Internet]. Rockville (MD): Substance Abuse and Mental Health Services Administration; 2015 Sep. Figure 33: alcohol use disorder in the past year among people aged 12 or older, by age group: percentages, 2002–2014; [cited 2017 Sep 5]. (HHS Publication No. SMA 15- 4927). Available from: https:// www.samhsa.gov/data/sites/ default/files/NSDUH-FRR1-2014/ NSDUH-FRR1-2014.htm#idtext anchor061 34 Mojtabai R, Olfson M, Sampson NA, Jin R, Druss B, Wang PS, et al. Bar- riers to mental health treatment: results from the National Comor-
- 52. bidity Survey Replication. Psychol Med. 2011;41(8):1751–61. 35 Wang PS, Berglund P, Olfson M, Pincus HA, Wells KB, Kessler RC. Failure and delay in initial treatment contact after first onset of mental disorders in the National Comor- bidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):603–13. 36 Han B, Gfroerer J, Kuramoto SJ, Ali M, Woodward AM, Teich J. Medicaid expansion under the Affordable Care Act: potential changes in receipt of mental health treatment among low- income nonelderly adults with seri- ous mental illness. Am J Public Health. 2015;105(10):1982–9. 37 Tai B, Volkow ND. Treatment for substance use disorder: opportuni- ties and challenges under the Af- fordable Care Act. Soc Work Public Health. 2013;28(3-4):165–74. 38 Han B, Compton WM, Mojtabai R, Colpe L, Hughes A. Trends in receipt of mental health treatment among adults in the United States, 2008– 2013. J Clin Psychiatry. 2016; 77(10):1365–71. 39 Substance Abuse and Mental Health Services Administration. National
- 53. Mental Health Services Survey, 2010 and 2014 [Internet]. Rockville (MD): SAMHSA; [cited 2017 Sep 6]. Avail- able from: https://wwwdasis .samhsa.gov/dasis2/nmhss.htm 40 Substance Abuse and Mental Health Services Administration. National Survey of Substance Abuse Treat- ment Services, 2008–14 [Internet]. Rockville (MD): SAMHSA; [cited 2017 Sep 6]. Available from: https:// wwwdasis.samhsa.gov/dasis2/ nssats.htm October 2017 36:10 Health Affairs 1747 o n O cto b e r 1 1 , 2 0 1 7 b y H W
- 55. rg / D o w n lo a d e d fro m http://content.healthaffairs.org/ Reproduced with permission of copyright owner. Further reproduction prohibited without permission.