
Recommended
More Related Content
Similar to RENAL CELL CARCINOMA .pptx
Similar to RENAL CELL CARCINOMA .pptx (20)
More from Sumantra Dey
Recently uploaded
Recently uploaded (20)
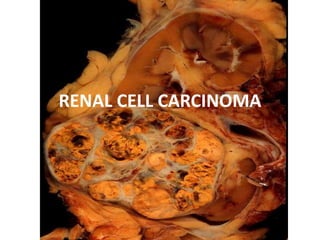
RENAL CELL CARCINOMA .pptx
- 2. • Also known as hypernephroma, internist tumour, gravitz tumour. Incidence- • RCC represents 2% of overall cancer incidence and mortality. • 85% of primary malignant tumour • M:F-2:1 • Commonly occurs in 6th decade of life
- 3. Etiology • Environmental exposure • RCC occurs in 2 forms- -inheritated -sporadic • 2 other forms of hereditary RCC -von-hippel lindau disease -papillary RCC • Higher in dialysis pt.
- 4. Pathology • Clear cell type-25% • Granular cell type-25% • Mixed type-rest%
- 5. Clear cell RCC • <5% multicentric or bilateral • 50% stage I & II at presentation • <5% stage IV • Organ involvement with metastases – 40% bone – 22% adrenals – 15% brain – 14% kidney
- 6. Papillary RCC • 70% stage I • More commonly bilateral and multifocal
- 7. Spread • Local • Blood • Lymphatic
- 8. Staging :The Robson staging system – Stage I - Tumor confined within renal parenchyma – Stage II - Tumor invading perinephric fat but still contained within the Gerota fascia – Stage III - Tumor invading the renal vein or inferior vena cava (A), or regional lymph-node involvement (B), or both (C) – Stage IV - Tumor invading adjacent viscera (excluding ipsilateral adrenal) or distant metastases
- 9. Staging :TNM – Primary tumor (T) • TX - Primary tumor cannot be assessed • T0 - No evidence of primary tumor • T1 - Tumor 7 cm or smaller in greatest dimension, limited to the kidney • T2 - Tumor larger than 7 cm in greatest dimension, limited to the kidney • T3 - Tumor extends into major veins or invades adrenal gland or perinephric tissues but not beyond the Gerota fascia • T3a - Tumor invades adrenal gland or perinephric tissues but not beyond the Gerota fascia • T3b - Tumor grossly extends into the renal vein(s) or vena cava below the diaphragm • T3c - Tumor grossly extends into the renal vein(s) or vena cava above the diaphragm • T4 - Tumor invading beyond the Gerota fascia
- 10. – Regional lymph nodes (N) - Laterality does not affect the N classification • NX - Regional lymph nodes cannot be assessed • N0 - No regional lymph node metastasis • N1 - Metastasis in a single regional lymph node • N2 - Metastasis in more than 1 regional lymph node – Distant metastasis (M) • MX - Distant metastasis cannot be assessed • M0 - No distant metastasis • M1 - Distant metastasis
- 11. Staging and Prognosis Cohen HT, McGovern FJ. NEJM. 2005;353:2477.
- 12. • AJCC stages – AJCC stage I - T1, N0, M0 – AJCC stage II - T2, N0, M0 – AJCC stage III - T1-2, N1, M0 or T3a-c, N0-1, M0 – AJCC stage IV - T4; or any T, N2, M0; or any T, any N, M1
- 13. C/F • M:F-2:1 • Hematuria • Lt sided varicocele • Triad –pain,hematuria,mass • Atypical presentation-25% • Persistent pyrexia with no evidence of infection • Constitutional symptoms
- 14. PARANEOPLASTIC SYNDROME • Polycythemia • 20% hypercalcemia • 40% HTN • Stauffers syndrome • Biological active products- -ACTH-cushing syndrome -enteroglucagon-protein enteropathy -prolactin-galactorrhoea -insulin-hypoglycemia -gonadotrophin-gynaecomastia and decrease libido
- 15. Investigation : • USG abdomen • IVP • CECT abdomen • Renal angiography • MRI • CXR • FNAC
- 16. • Complete blood count • Urine examination • KUB x-rays
- 17. • Anemia occurs in 30% of RCC • Anemia is not secondary to blood loss or hemolysis and is normochromic. • Gross hematuria is seen upto 60% • ESR • Calcium level • LFT • detectable calcification or is large enough to distort the normal renal contour.
- 18. • IVP used alone75% accurate. • Calcification overlying the renal shadow is an important finding. • USG –non invasive, inexpensive, able to delineate a renal mass seen on IVU. Approx 98% accurate. • Extension of tumor thrombus into IVC can also be determined.
- 19. • CECT abdomen – Diagnosis – Staging – Renal Angiography
- 20. • More sensitive than US / IVU • Typical finding of a mass that becomes enhanced with the use of IV contrast. • Amputation of a portion of the collecting system,presence of calcification, poorly defined interface between renal parenchyma and lesion. • Method of staging by visualizing renal hilum, perinphric space, renal vein, IVC, adrenals, regional LN, adjacent organs.
- 21. Typical renal cell carcinoma. CT scan obtained before contrast enhancement
- 22. Typical renal cell carcinoma. Contrast-enhanced CT
- 23. Treatment • Localised disease-surgical removal • Radical nephrectomy is primary treatment • Pre-operative renal artery embolisation can be used as adjuvant therapy to facilitate radical nephrectomy. • Radiation therapy • Different approach-midline ,thoraco abdominal,classsical lumbar incision
- 24. • Partial nephrectomy • Laparoscopic nephrectomy
- 26. Partial nephrectomy performed Intraoperative View Specimen (Renal Cell Carcinoma) Fisse
- 27. Indications for nephron-sparing surgery (NSS) • Absolute – nephrectomy would render patient anephric – bilat tumours, solitary kidney, familial RCC • Relative – Future threat to contralateral kidney • Elective – Small, exophytic, polar location – Benign disease
- 28. Disseminated disease • About 30%pt present with disseminated RCC • Radical nephrectomy _as a palliative treatment • Radiation therapy • Hormonal therapy • Biologic response modifiers
- 29. Prognostic factors • 5-year survival • By stage – T1 - 80%-100% – T2-3a – 60% – T3b – 15-20% – T4 – 0-20%
- 31. Bosniak classification of renal masses is as follows: class I includes simple cysts; class II, minimally complicated but overwhelmingly benign masses with thin septa, hyperattenuation, or small amounts of mural or septal calcification; class III, moderately complicated masses with mural nodularity, thick septa, or irregular or thick calcifications that often require surgical exploration; class IV, significantly complicated and generally malignant masses with thick and irregular enhancing regions and definite solid components.