Ronan Herlihy on Engaging Clinicians with data on their ordering practices
Presentation_1048
1. Together, our Promise is YOUR HEALTH.
LRH is committed to continuous improvement and in October
2013 a project to improve Patient Readiness for surgical cases
was initiated. Patient Readiness is important as it promotes the
safety of the patient, decreases delays, and improves the overall
experience of the patient through their continuum of care.
Lakeland Regional Health is a full service medical center and health system. As an 851 bed, not for profit medical
center, Lakeland Regional Health (LRH) is the fifth largest hospital in the state of Florida and also operates the busiest
single-site Emergency Department in the state. LRH has an average surgical case volume of over 1400 cases per month.
IMPROVING PATIENT READINESS:
Increasing patient safety and operating room efficiency
RESULTS & IMPLICATIONS
KEYS TO SUCCESS
Patient Readiness is defined by LRH as having all documents and physician orders
required for an elective surgery to be received by twelve noon the business day
prior to the surgery date. Documents include History and Physical, Consent,
Electrocardiograms, Labs, Medical Clearance, Cardiac Clearance, etc.…. Initial
baseline metric for patient readiness at project start was 41% in October 2013 and
as a result of process and policy redesign we have currently achieved and sustained
over 80% each month since October 2014. In order to obtain metrics needed for
analysis, a tracking board was utilized by the Pre-Admit Testing department to mark
the date and time of when patient readiness documents and physician orders were
received. In addition, at twelve noon the day prior to surgery, any remaining charts
that were missing documents were checked again to determine if the patient’s chart
was to be marked complete or incomplete on the tracking board. The project team
utilized the metrics to provide physicians and their offices a scorecard which showed
them the percent of their cases that were complete and met the patient readiness
goal and the details of when each document required for the patient to have surgery
was received by the Pre Admission Testing Department. A process hard-stop was
initiated if documents and orders were not received for elective cases by twelve
noon the business day prior to scheduled surgery date. If the case was marked
incomplete by the Pre-Admission testing department it was sent to surgery
leadership to determine if the case should be rescheduled. Pre-Admission testing
also sends out reminder notifications to offices and physicians at 48 hours and 24
hours prior to scheduled surgery date in order to remind physicians and offices to
send in their documents and place their orders on time.
Objectives
DESIGN
PARTICIPANTS
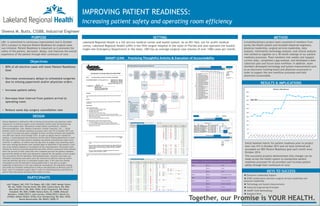
SMART LEAN: Practicing Thoughtful Activity & Execution of Accountability
PURPOSE SETTING METHOD
• 80% of all elective cases will meet Patient Readiness
Goal
• Decrease unnecessary delays to scheduled surgeries
due to missing paperwork and/or physician orders
• Increase patient safety
• Decrease time interval from patient arrival to
operating room
• Reduce same day surgery cancellation rate
Initial baseline metric for patient readiness prior to project
start was 41% in October 2013 and we have achieved and
exceeded our 80% Patient Readiness goal each month since
October 2014.
This successful projects demonstrates that changes can be
made across the health system to standardize patient
readiness processes for all providers and increase patient
safety through their continuum of care.
A multidisciplinary project team consisted of members from
across the health system and included industrial engineers,
physician leadership, surgical services leadership, data
analysts, information technology analysts, and clinical analysts
who worked to together on a 18 month redesign of our patient
readiness processes. Team members met weekly and mapped
current state, completed a gap analysis, and developed a date
collection plan and future state workflow. In addition, team
members developed technology and system improvements such
as an electronic tracking board and physician scorecards in
order to support the new workflow processes and hold
physicians accountable.
Executive Leadership Support
DYAD collaboration between surgical services leadership and
physician leadership
Technology and System Improvements
Industrial Engineering Principles
SMART LEAN Methodology
Standard Work
PAT Patient Readiness Tracking Process Flow (draft 9.8.14)
End
Start
HUC receives
items on fax server
or through red
envelope courier
for patient chart
and names files
(Patient Name &
Surgery Date)
Is patient chart
complete? All items
have been received
AND orders are
present
HUC creates and/or
adds to already
created patient chart
with items that have
been received and
marks tracking board
that items have been
received
HUC places
patient chart in
queue for RN to
review
RN reviews chart
including orders
and makes any
changes to
tracking board if
necessary
(including
backdating)
RN marks Chart
Complete on
tracking board
and places chart in
file or on cart
Is patient scheduled
for surgery the next
day?
RN reviews any
Incomplete chart
starting at 12 noon the
day prior and reviews
chart including orders
and makes any changes
to tracking board if
necessary
(including backdating).
Is patient chart
complete? All items
have been received
AND orders are
present
RN marks Chart
Complete on tracking
board and places
chart on cart
RN marks Chart
Incomplete on
tracking board and
marks any missing
item as incomplete on
tracking board and
places chart on cart
Delay for review
(patient folder
placed in file or
on cart)
NOTES:
· HUC will not review parameters
of EKG
· Nurse will call (and/or email,
tbd..) doctor’s offices to remind
them of missing items
· Nurse is responsible for
reviewing all patient readiness
items for accuracy
· Tracking Board automatically
documents initials of who
checked item for internal review
Is patient scheduled
for surgery < 48
hours?
RN creates patient
chart
Y
N Y
N
N
Y
N
Y
Notification reminder
sent to physician and
their office at 24 hours
prior to scheduled
surgery date with details
on what items are
missing
Jack Thigpen, MD, CSO; Tim Regan, MD, CQO, CMIO; Margie Voyles,
RN, MS, CNOR; Cheryle Smith, RN, MSN; Cateria Davis, RN, BSN;
Mary Beth Perry, RN, MSN, CPAN; Cindy Fitzpatrick, RN; Diane
Campbell, RN, MSN, CSSBB; Sheena Butts, IE, CSSBB; Deborah
Newbern, CHAM,CRCE-I; Jane Carlson, CHAM,CRCE-I; Derek Cyr,
CPHIMS; Debbie Walker, RT(R); Ever Glendenning, RN, BSN, CPAN;
Renee Mountcastle, RN, BSAST, CNOR, IT
Sheena M. Butts, CSSBB, Industrial Engineer
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Patient Readiness
GOAL: 80%