Top profile Call Girls In Sagar [ 7014168258 ] Call Me For Genuine Models We ...
8 PE OF THE GENITOURINARY.pdf
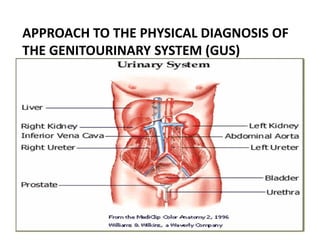
1. APPROACH TO THE PHYSICAL DIAGNOSIS OF
THE GENITOURINARY SYSTEM (GUS)
12/30/2016 1
Muhammed GUS
2. INTRODUCTION
• This system is more dependent than most on
laboratory, histopathology and imaging techniques
for completion of the diagnostic process.
• The basic principles of clinical assessment,
however, still apply; appropriate and careful history
taking and physical examination are essential and
can often lead to a diagnosis.
12/30/2016 2
Muhammed GUS
3. History should be taken in detail. if the pt is female:
• age at menarche, number of deliveries,
• complications at pregnancy or delivery should be
documented.
There is still unwarranted stigma and shame
attached to STD.
The interview and examination must be carried out
in privacy and with confidentiality.
As with other clinical problems, diagnosis is
achieved by history, examination and relevant
investigation
12/30/2016 3
Muhammed GUS
4. Anatomy and Physiology Review
• Kidneys
• Ureters
• Urinary bladder
• Urethra
12/30/2016 4
Muhammed GUS
5. Function of the Urinary System
• The primary function of the urinary system is
Maintain homeostasis
Regulate fluids and electrolytes
Eliminate waste products
Maintain BP
Involved with RBC production
Involved with bone metabolism
12/30/2016 5
Muhammed GUS
6. Kidneys
• Paired
• Located retroperitoneally on the posterior wall of
the abdomen from T12-L3
• The average adult kidney weighs 4.5 oz/127.5 gm
• The right kidney sits lower in the abdomen due to
liver placement
• An adrenal gland sits on top of each kidney
12/30/2016 6
Muhammed GUS
7. Kidney…
Each kidney has two parts
• The renal medulla is the inner portion
– consists of renal pyramids which are collecting
ducts that drain into renal pelvis
– Once urine leaves the renal pelvis the
composition or amount of urine does not change
• The Cortex is the outer portion
– contains nephrons
12/30/2016 7
Muhammed GUS
9. Nephron
• Each kidney has approximately 1 million
nephrons
• If the function is less than 20% replacement
therapy is usually initiated
• The nephron is responsible for the initial
formation of urine
12/30/2016 9
Muhammed GUS
10. KIDNEY FUNCTIONS
• Urine formation
• Excretion of waste products
• Regulation of electrolytes
• Regulation of acid-base balance
• Control of water balance
• Control BP
• Regulation of RBC production
• Synthesis of vitamin D to active form
• Secretion of prostaglandins
• Regulation of calcium and phosphorus balance
12/30/2016 10
Muhammed GUS
11. Urine Formation
• Urine is formed in the nephrons in a three step
process
– Glomerular filtration
– Tubular reabsorption
– Tubular secretion
• Glomerular Filtration produces ultrafiltrate which
enters the tubules
• Selective reabsorption of H2O & solutes occurs in
tubules
• Selective secretion of solutes occurs in tubules
• 99% of ultrafiltrate is reabsorbed into the
bloodstream
• 1000-1500mL of urine is produced each day
12/30/2016 11
Muhammed GUS
12. Excretion of Waste Products
• The kidney is the body’s main excretory organ
• The major waste product of protein metabolism is
urea
– 25-30g are produced and excreted daily
• Other waste products include:
– Creatinine
– Phosphates
– Sulfates
– Uric acid
– Drug metabolites
12/30/2016 12
Muhammed GUS
13. Regulation of Electrolytes
• In normally functioning kidneys the amount of
electrolytes excreted per day is equal to the
amount ingested
• Sodium
– Linked to blood volume and pressure
– 90% of Na in ultrafiltrate is reabsorbed in the
proximal tubules and loops of Henle
– Aldosterone causes kidneys to reabsorb sodium
• Potassium
– The kidneys excrete more than 90% of K intake to
maintain a normal serum balance
– Aldosterone causes the kidneys to excrete potassium
12/30/2016 13
Muhammed GUS
14. Regulation of acid-base balance
• Normal serum pH is 7.35-7.45
• Normal urine pH is 4.6-8
• Kidneys 3rd line of defense in acid-base balance
– respiratory & other buffer systems respond more
rapidly
– kidneys require several hours to a day or more to
readjust balance
• Reabsorb bicarbonate from ultrafiltrate
• Excrete large quantities of acid in the urine
(phosphoric and sulfuric acids) by buffering with
ammonia
12/30/2016 14
Muhammed GUS
15. Control of water balance
• The human body is made up of 60% water
• Regulated by Antidiuretic hormone (ADH) or vasopressin
• Secreted by the posterior pituitary in response to serum
osmolality
• ADH increases reabsorption of water to return serum
osmolality to normal
• Decreased water intake stimulates ADH release
• ADH controls volume & concentration of urine by
regulating permeability of distal tubule to H2O
12/30/2016 15
Muhammed GUS
16. Control BP
• The kidney secrets the hormone renin when there is
a decrease in BP
• Renin converts angiotensinogen to angiotensin I
• Angiotensin I converts to angiotensin II
• Angiotensin II is a powerful vasoconstrictor and
causes BP to increase
• Increase in BP stops the excretion of renin
• The adrenal cortex also releases aldosterone in
response to increasing serum osmolality or poor
perfusion to increase BP
12/30/2016 16
Muhammed GUS
17. Regulation of RBC production
• The kidneys release erythropoietin when they
sense a decrease in oxygen in the blood
• Erythropoietin stimulates the bone marrow to
produce RBCs
Vitamin D Synthesis
• The kidneys convert inactive vitamin D to 1,25-
dihydroxycholecalciferol
• Vitamin D is necessary for calcium balance
12/30/2016 17
Muhammed GUS
18. Ureters
• 1 ureter per kidney
• Long fibromuscular tubes that connect each
kidney to the bladder
• Enter bladder at an oblique angle to prevent
flow blockage
• Propel urine to bladder through peristalsis
12/30/2016 18
Muhammed GUS
19. Bladder
• Hollow, muscular organ behind the pubic bone
• Anatomic capacity is 1500-2000mL
• Wall of the bladder contains four layers
–Adventitia—Outer layer/connective tissue
–Detrusor—smooth muscle
–Submucosal layer—loose connective tissue
–Mucosal lining—Inner layer/impermeable to
water
• Bladder neck forms Internal sphincter which is
composed of smooth muscle
12/30/2016 19
Muhammed GUS
20. Urethra
• Female = 4 cm; Opens anterior to the vagina
• Male = 20 cm; 3 sections
–Prostatic: superior end joins bladder &
internal involuntary sphincter;
–dilatable at this point & larger;
–has 2 ejaculatory ducts
12/30/2016 20
Muhammed GUS
21. SYMPTOMS OF GENITOURINARY DISEASES
Urinary Tract
A. Renal pain: pain arising from the kidneys and
is usually felt at or below the costal margin posteriorly.
may radiate anteriorly towards the umbilicus
is typically dull aching and steady
Kidney pain occurs in acute pyelonephritis
B. Ureteric pain: Results from sudden distention of the
ureter and associated distention of the renal pelvis.
It is severe colicky pain which originates in the
costovertebral angle.
It may radiate into the lower quadrant of the abdomen and
possibly to the upper thigh and testicle
12/30/2016 21
Muhammed GUS
23. C. Hematuria: Is the presence of red blood cells in the urine.
It is a lab diagnosis.
Reddish discoloration of urine may be due to the presence
of pigments in the urine.
Can be continuous or intermittent and may be associated
with pain.
D. Oliguria: Denotes the passage of less than 400 ml of urine
per day.
E. Anuria: Is the complete absence of urine output.
Retention of urine should be excluded before a pt is
considered to have anuria.
F. Polyuria: Implies a high urine output.
It is an arbitrary definition, on the basis of 24 hours urine
output of more than 3L per day.
G. Urinary frequency: Is an abnormally frequent voiding.
12/30/2016 23
Muhammed GUS
24. H. Nocturia: Implies the need to rise during hrs of
sleep to empty the bladder.
I. Dysuria: Is pain immediately before, during or
immediately after micturation.
J. Urgency: Is the loss of the normal ability to
postpone micturation beyond the time when the
desire to pass urine is initially perceived.
K. Incontinence: Refers to an involuntary loss of urine
that has become a social or hygienic problem
L. Hesitancy: Is difficulty initiating the process of
micturation
M. Terminal dribbling: is difficulty of completing
micturation in a clean stop fashion
12/30/2016 24
Muhammed GUS
25. The Male Genital Tract
• Urethral discharge: is nearly always a complaint
of men, in the form of
dripping
staining of the underwear
The color, amount and duration of the discharge
have to be ascertained.
Commonest causes are sexually transmitted
infections. It can be grouped as:
Gonococcal urethritis
Non-gonococcal urethritis
12/30/2016 Muhammed GUS 25
26. • Genital ulcer: This may be recurrent, single or
multiple, painful or painless.
It is important to ascertain the evolution of the ulcer.
Common causes include
chancre of primary syphilis
chancroid
genital herpes
Other complaints
• History of sores, growths on the penis
• History of swelling or pain in the scrotum
• Past history of sexually transmitted infections
• History of sexual dysfunction
12/30/2016 Muhammed GUS 26
27. The Female Genital Tract
• Vaginal discharge
• can be associated with itching
• the color, odor and amount should be characterized
• Menstrual History: Various aspects should be
considered including:
• Regularity
• Age at menarche (age at first onset)
• Last menstrual period
• Length of time b/n periods
• How heavy is the flow
Estimate based on the number of pads or tampons
used daily
• Bleeding between periods
• History of pain during periods and severity, duration
of the pain
12/30/2016 Muhammed GUS 27
28. • Sexual History: may be obtained after winning the
pt’s confidence.
The history should include:
Date of last sexual contact, details of contacts over
recent months, possibility of homosexual and
bisexual contact and the type of sexual
The use of condoms should be enquired into
irrespective of whether the pt is using other methods
of contraception.
Psychosexual problems, including erectile
dysfunction and premature ejaculation
• Dyspareunia: Is pain on sexual intercourse.
It can be superficial (i.e. pain in the vulvovaginal
area) or
deep (pain deep in the vagina)
12/30/2016 Muhammed GUS 28
29. Physical examination
Kidneys
• Inspect the flanks for bruising or swelling
• Assess each kidney for tenderness.
Have the pt sit, then place the palm of your hand over the
costovertebral angle (CVA) and strike your hand with the
ulnar surface of the fist of your other hand.
Direct percussion with the fist over the CVA is also
acceptable.
The test should not cause any tenderness. If there is
tenderness it can be indicated as costo- vertebral angle
tenderness.
• Palpation of the kidneys may be carried out along with the
abdominal examination.
12/30/2016 Muhammed GUS 29
31. Physical examination…
Bladder
• Inspect the lower abdomen (suprapubic area). and
• palpate for enlarged bladder arising from the
pelvis
• Look for enlargement or distention.
• Palpate for tenderness or rigidity.
12/30/2016 Muhammed GUS 31
32. Genital Examination
• Male
• The Penis
• Note if circumcised. If not, is the foreskin easy to
retract?
• Check the external meatus of the urethra for any
discharge.
• Palpate the ventral aspect of the shaft for
tenderness or lesions e.g. cord like feeling of the
penile urethra in pts with urethral stricture
involving the bulbar urethra.
• Inspect for abnormal meatal opening
12/30/2016 32
Muhammed GUS
34. Scrotum
• The left testicle / scrotum usually hangs lower.
• Sebaceous cysts are a common lump found on the skin.
• Scrotal skin should be looked at for any redness, swelling
or ulcer. The posterior surface should also be inspected.
• If intrascrotal swelling is present considered the
following factors:
Observe whether it appears to extend into the groin and
note whether both testes are in the scrotum.
Is it possible to get above the mass?
Can the testis be palpated separately? Is it reducible?
Auscultation can also be carried out.
Masses should be further characterized with respect to
size, consistency, tenderness
12/30/2016 34
Muhammed GUS
36. Testes:
• Check by palpating using the thumb and first
two fingers. They should feel
• Smooth, rubbery, but free of nodules.
• The size and consistency of the testis and any
nodules or irregularities should be noted.
The epididymis:
• Should be smooth, discrete, and non-tender
• In acute epididymitis, it is tender, swollen and
may be difficult to distinguish from the testis.
• Palpate for the spermatic cord; look for
varicocele
12/30/2016 36
Muhammed GUS
39. • Prostate: Digital rectal examination will help assess
the size, consistency, tenderness and invasion of the
mucosa.
Female: Women are best examined in the lithotomy
position.
• The vulva, labia minora and majora are examined for
discharge, redness, swelling, excoriation, ulcers,
warts and other lesions.
• The labia are separated to palpate the Bartholin’s
glands, which are not normally palpable.
• A bivalve speculum is then inserted and the color of
the vaginal wall inspected and discharges, if
present, characterized with respect to color, odor
and consistency.
12/30/2016 39
Muhammed GUS
41. • The cervix is inspected for possible discharge, warts,
ulcers and ectopy.
• Having removed the speculum, the urethral orifice is
examined for discharge, inflammation and warts.
• Digital examination
Lubricate the index and middle fingers of your
gloved right hand.
From a standing position, insert them into the
vagina.
Note any nodularity or tenderness in the vaginal
wall.
Palpate the cervix-note its shape, position,
consistency, regularity, mobility or tenderness
Palpate the uterus b/n the hand in the pelvis and
your other hand placed on the abdomen.
12/30/2016 41
Muhammed GUS
42. Recto-vaginal examination
Withdraw your fingers. Lubricate your gloves again if
necessary.
Then slowly reintroduce your index finger into the
vagina, your middle finger into the rectum.
Ask the pt to strain down as you do this so that her
anal
sphincter will relax.
Recto-vaginal palpation is especially valuable in
assessing a retrodisplaced uterus
12/30/2016 42
Muhammed GUS