
Recommended
More Related Content
Similar to TYPHOID.pptx
Similar to TYPHOID.pptx (20)
More from Dr Pushkar Kumar
Recently uploaded
Recently uploaded (20)
TYPHOID.pptx
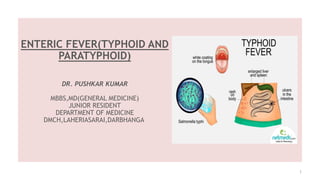
- 1. ENTERIC FEVER(TYPHOID AND PARATYPHOID) DR. PUSHKAR KUMAR MBBS,MD(GENERAL MEDICINE) JUNIOR RESIDENT DEPARTMENT OF MEDICINE DMCH,LAHERIASARAI,DARBHANGA 1
- 2. ETIOLOGY • Enteric Fevers are caused by infection with Salmonella enterica serotypes Typhi and Paratyphi A,B and C 9/3/2023 2
- 3. RISK FACTORS 9/3/2023 3 Individuals on frequent use of Antacids,H2 Blockers or PPI or advanced age with achlorhydria,post- gastrectomy status are at high risk. Acid medium with pH level of 1.5 or less kills most of the bacilli
- 4. PATHOGENESIS 9/3/2023 4 • Mode of transmission- Faeco-oral route through contaminated food/water • Salmonella organisms penetrate the mucosa of both small and large bowel and proliferate intracellularly • Organisms invade and replicate in macrophages in peyer's patches,mesenteric lymphnodes,liver,spleen • There are four phases in the evolution of pathology of eneteric fever. • Huckstep's Four Phases : • 1.Hyperplasia of lymphoid follicles • 2.Necrosis of the lymphoid follicles in the second week involving both mucosa and sub-mucosa • 3.Longitudinal Ulceration of the bowel with the possibility of perforation and hemorrhages • 4.Healing takes place from the 4th week onward (Longitudinal ulcers heal without fibrosis/stricture in contrast to tubercular ulcers which heal with fibrosis/stricture
- 5. 9/3/2023 5
- 6. TUBERCULAR ULCERS Vs TYPHOID ULCERS 9/3/2023 6
- 8. ROSE SPOTS ON THE CHEST OF A PATIENT WITH ENTERIC FEVER 9/3/2023 8
- 9. 9/3/2023 9 Paratyphoid fever course tend to be shorter that that of typhoid fever and onset is often more abrupt with acute enteritis The rash may be more abundant and complication less frequent
- 10. INVESTIGATIONS • 1st week – Blood picture And Blood culture (gold standard) • Leukopenia occurs with eosinopenia and relative lymphocytosis • Blood cultures are positive for S. enterica subsp. enterica serovar Typhi • 2nd week- The Widal test is strongly positive, with antiO and antiH antibodies • 3rd week- Stool culture • 4th week-Urine culture 9/3/2023 10
- 12. 9/3/2023 12
- 13. NEW DIAGNOSTIC TESTS 9/3/2023 13 IDL tubex test – Detects IgM09 antibodies in few minutes. Typhidot test – Detects IgM & IgG antibodies.
- 14. MANAGEMENT • Medical management : Antibiotic Therapy • Fluoroquinolones are the drugs of choice (e.g. ciprofloxacin 500 mg twice daily for 14 days) • Cephalosporins are alternatives- Ceftriaxone 1g IV bd or Cefixime but are associated with high treatment failure rate • Azithromycin 1g/day- indicated in quinolones resistance • Ampicillin, chloramphenicol, trimethoprim-sulphamethoxazole and amoxicillin can also be used • Multi-Drug resistance- Resistance to Chloramphenicol,cotrimoxazole and ampicillin • Xtremely Drug resistance cases reported from Pakistan- Resistance to quinolone and ceftriaxone 9/3/2023 14
- 15. SURGICAL MANAGEMENT • Surgery is usually indicated if intestinal perforation occurs • Most surgeons prefer simple closure of the perforation with drainage of the peritoneum. Small-bowel resection is indicated for patients with multiple perforations. • If antibiotic treatment fails to eradicate the hepatobiliary carriage, Cholecystectomy is sometimes successful, especially in patients with gallstones, but is not always successful in eradicating the carrier state because of persisting hepatic infection. 9/3/2023 15
- 16. COMPLICATIONS 16 9/3/2023 Gastro-intestinal- mainly Intestinal Haemorrhage Terminal ileal perforation Peritonitis Acute cholecystitis Hepatitis
- 17. CHRONIC CARRIER STATE 9/3/2023 17 • After clinical recovery, about 5% of patients become chronic carriers (i.e. continue to excrete the bacteria after 1 year) • Bacilli may live in the gallbladder for months or years and pass intermittently in the stool and, less commonly, in the urine • Fecal carriers – Most common • Healthy carriers – Emerge from subclinical cases • Urinary carriers – More dangerous, common in patients with calculi or schistosomiasis. • More common in women, infants, older age groups (> 40 years) and biliary abnormalities. • Treatment- 4 weeks with ciprofloxacin but may require an alternative agent and duration, as guided by antimicrobial sensitivity testing
- 19. PREVENTION • Improved sanitation and living conditions reduce the incidence of typhoid. • It can spread only in environments where human feces can come into contact with food or drinking water • Travellers to countries where enteric infections are endemic should receive typhoid vaccination. • Vaccine- Multiple dose oral/single dose parenteral • Live oral attenuated- Ty21a- On Day 1,3 and 5 • Can be given to adults and children above 6 yrs of age and contraindicated in pregnancy • Parenteral-Vi polysaccharide • A single dose of 0.5 ml/25 microgram as s/c or im can be given to all above 2 yrs of age • Booster dose should be given every two years 9/3/2023 19
- 20. THANK YOU !! 9/3/2023 20