
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Cardiomyopathy Guide
Similar to Cardiomyopathy Guide (20)
Recently uploaded
Recently uploaded (20)
Cardiomyopathy Guide
- 2. KRISHNA INSTITUTE OF NURSING SCIENCES KARAD SUBJECT:- MEDICAL SURGICAL NURSING TOPIC:- CARDIOMYOPATHY, DILATED, RESTRICTIVE, HYPERTROPHIC PRESENTED BY:- MS.POOJA MHALATKAR 2ND YEAR MSC(N) KINS KARAD
- 3. GENERAL OBJECTIVES At the end of the class the student will be able to get detailed knowledge regarding the cardiomyopathy (dilated, restrictive, hypertrophic).
- 4. SPECIFIC OBJECTIVES • At the end of the class the student will be able to: • Define the cardiomyopathy. • Explain the different types of cardiomyopathy. • Explain about the pathophysiology • List down the causes, signs and symptoms of cardiomyopathy.
- 5. • Enlist the risk factors, and its complications of cardiomyopathy. • Mention the different Diagnostic tests. • Discuss about the medical, nursing and surgical management • prevention
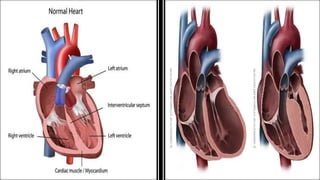
- 6. INTRODUCTION The term “cardiomyopathy” refers to “cardio” (heart), “myo”(muscle), “pathy” (diseases of). Cardiomyopathy is a diseases of the heart muscles that makes it harder for your heart to pump blood to the rest of your body. Cardiomyopathy can lead to heart failure.
- 7. The main types of cardiomyopathy include dilated hypertrophic and restrictive cardiomyopathy. Treatment which might include medications, surgically implanted devices or, in severe cases, a heart transplant depends on which type of cardiomyopathy you have and how serious it is.
- 8. DEFINITION Cardiomyopathy is a diseases of the heart muscle that makes it harder for your heart to pump blood to the rest of your body. Cardiomyopathy can lead to heart failure. The main types of cardiomyopathy include dilated, hypertrophic and restrictive cardiomyopathy.
- 9. TYPES OF CARDIOMYOPATHY There are three main types of cardiomyopathy. Dilated, hypertrophic and restrictive. In dilated cardiomyopathy, the ventricles are enlarge. In hypertrophic cardiomyopathy, walls of the ventricles thicken and become stiff. In restrictive cardiomyopathy, the walls of ventricles become stiff, but not necessarily thickened.
- 10. DILATED CARDIOMYOPATHY:- In dilated cardiomyopathy, the size of the ventricle cavity enlarges with reduced cardiac output. Contractile function decreases as the myocardial tissue is destroyed. Blood moves more slowly through the left ventricle, which often results in blood clot formation.
- 11. Dilated cardiomyopathy is the most frequent type of cardiomyopathy and one of the most frequent causes of heart failure. Dilated cardiomyopathy may be hereditary, follow infectious myocarditis, or be caused by chronic alcohol or cocaine use, HIV, thiamine or zinc deficiences, infections or other causes.
- 13. HYPERTROPHIC CARDIOMYOPATHY:- Hypertrophic cardiomyopathy is enlargement of the cardiac muscle wall, often of the septum (asymmetrical septal hypertrophy) and less common left ventricle (ventricular hypertrophy). Hypertrophic cardiomyopathy causes the ventricle wall to be rigid, which decreases ventricular filling.
- 14. If an enlarged septum obstructs the outflow of blood through the aortic valve, it is known as obstructive hypertrophic cardiomyopathy due to asymmetrical septal hypertrophy.
- 16. RESTRICTIVE CARDIOMYOPATHY:- Restrictive cardiomyopathy impaires ventricular stretch and limits ventricular filling. Cardiac muscle stiffness is present with no ventricular dilation, although systolic emptying of the ventricles remains normal.
- 17. restrictive cardiomyopathy is the rarest form of cardiomyopathy. It may be caused by infiltrative diseases such as amyloidosis that deposit the protein amyloid within the myocardial cells, making the muscle stiff and resistant to stretching for easy ventricular filling.
- 19. CAUSES PRIMARY CARDIOMYOPATHY:- Refers to those conditions in which the etiology of the heart diseases is unknown (idiopathic). The heart muscle in this case is the only portion of the heart involved, and other cardiac structures are unaffected.
- 20. SECONDARY CARDIOMYOPATHY:- The cause of the myocardial diseases is known and is secondary to another disease process.
- 21. CAUSES OF SECONDARY CARDIOMYOPATHY • Cardiotoxic agents:- alcohol, cocaine, doxorubicin (Adriamycin) • Genetic (autosomal dominant) or familial • Ischemia (coronary artery diseases) • Muscular dystrophy • Hypertension • Metabolic disorders • Myocarditis
- 22. • Pregnancy • Aortic stenosis • Amyloidosis • Neoplastic tumor • Valve disease • Endomyocardial fibrosis • Ventricular thrombus
- 24. SIGNS AND SYMPTOMS There might be no signs or symptoms in the early stages of cardiomyopathy. But as the condition advances, signs and symptoms usually appear, including:- Breathlessness with exertion or even at rest. Swelling of the legs, ankles and feet. Bloating of the abdomen due to fluid buildup
- 25. Cough while lying down Fatigue Heartbeats that feel rapid, pounding or flutering Chest discomfort or pressure Dizziness, lightheadedness and fainting.
- 26. RISK FACTORS There are a number of factors that increase your risk of cardiomyopathy, including:- Family history of cardiomyopathy, heart failure and sudden cardiac arrest Long term high blood pressure Conditions that affect the heart, including a past heart attack, coronary artery diseases or an infection in the heart( ischemic cardiomyopathy).
- 27. Obesity, which makes the heart work harder Long term alcohol abuse. Illicit drug use, such as cocaine, amphetamines and anabolic steroids. Certain diseases, such as diabetes, an under or overactive thyroid gland, or disorder that causes the body to store excess iron ( Hemochromatosis).
- 28. Other conditions that affect the heart, such as a disorder that causes the buildup of abnormal proteins (amyloidosis), a diseases that causes inflammation and can cause lumps of cells to grow in the heart and other organs (sarcoidosis), or connective tissue disorders.
- 29. COMPLICATIONS Cardiomyopathy can lead to other heart conditions, including:- HEART FAILURE:- Your heart can’t pump enough blood to meet your body needs. Untreated, heart failure can be life threathening. BLOOD CLOTS:- Because your heart can’t pump effectively, blood clots might form in your heart. If clots enter your bloodstream, they can block the blood flow to other organs, including your heart and brain.
- 30. VALVE PROBLEMS:- Because cardiomyopathy causes the heart to enlarge, the heart valves might not close properly. This lead to a backward flow of blood. CARDIAC ARREST AND SUDDEN DEATH:- Cardiomyopathy can lead to abnormal heart rhythms. These abnormal heart rhythms can result in fainting or, in some cases, sudden death if your heart stops beating effectively.
- 31. DIAGNOSTIC TESTS Cardiomyopathy is seen on a chest x-ray examination. Echocardiography shows muscle thickness and chamber size to differentiate between the types of cardiomyopathy Changes related to enlarged chamber size, tachycardia and dysrhythmias can be seen on the ECG.
- 32. Cardiac catheterization with angiocardiography may also be useful. Cardiovascular magnetic resonance is a newer tool that is being used that has greater accuracy in diagnosing cardiomyopathy.
- 33. MEDICAL MANAGEMENT Medical management is directed toward determining and managing possible underlying or precipitating causes correcting the heart failure with medications, a low sodium diet, and an exercise rest regimen and controlling dysrhythmias with antiarrhythmic medications and possibly with an implanted electronic device, such as implantable cardioverter- defibrillator.
- 34. If patients exhibits signs and symptoms of congestion, their fluid intake may be limited to 2 liters each day. The person with HCM may also have to limit physical activity to avoid a life threathening dysrhythmia. A pacemaker may be implanted to alter the electrical stimulation of the muscle and prevent the forceful hyperdynamic contractions that occurs with HCM.
- 35. NURSING MANAGEMENT IMPROVING CARDIAC OUTPUT:- Monitor heart rate, rhythm, temperature and respiratory rate at least every 4 hours. Evaluate CVP, pulmonary artery wedge pressure, by pulmonary artery catheter to assess progress and effect of drug therapy. Calculate cardiac output, cardiac index and systemic vascular resistance.
- 36. Observe for changes in CO, such as depressed BP, change in mental status, decreased output. Administer pharmacologic support as directed, and observe for changes in hemodynamic and clinical status. Administer medications to control or eradicate dysrhythmias as directed. Administer anticoagulations as directed, especially for patients in artrial fibrillation.
- 37. REDUCING FATIGUE:- Make sure that patient and visitors understand the importance of rest. Assist patient in identifying stressors and reducing their effect (important for patients with hypertrophic cardiomyopathy because stress worsens the outflow obstructions).
- 38. Provide uninterrupted periods, and assist with ambulation as ordered. Teach the use of diversional activities and relaxation techniques to relieve tension.
- 39. HEALTH EDUCATION:- Teach about medications such as digoxin. Take daily only after taking pulse; notify doctor if pulse is below 60beats/minute. Report signs of digoxin toxicity anorexia, nausea and vomiting. Follow-up for periodic blood levels. Advise to take low sodium diet. Advice reporting signs of heart failure weight gain, edema, shortness of breath, increased fatigue.
- 40. SURGICAL MANAGEMENT When heart failure progresses and medical treatment is no longer effective, surgical intervention, including heart transplantation, is considered. However, because of the limited number of organ donors, many patients die waiting for transplantation.
- 41. In some cases, a left ventricular assist device(LVAD) is implanted to support the failing heart until a suitable donor heart becomes available mechanical assist devices and total artificial hearts.
- 42. LEFT VENTRICULAR OUTFLOW TRACT SURGERY:- When a patient with HCM becomes symptomatic despite medical therapy and a difference in pressure of 50mm Hg or more exists between the left ventricle and the aorta, surgery is considered. The most common procedure is a myectomy (sometimes referred to as a myotomy- myectomy), in which some of the heart tissue is excised.
- 43. Septal tissue approximately 1 cm wide and deep is cut from the enlarged septum below the aortic valve. The length of septum removed depends on the degree of obstruction caused by the hypertrophied muscle. Instead of a septal myectomy, the surgeon may open the left ventricle outflow tract valve to the aortic valve by removing the mitral valve, chordae, and papillary muscles.
- 44. The mitral valve then is replaced with a low profile disk valve. The space taken up by the mitral valve is substantially reduced by the prosthetic valve compared with the patients own valve, chordae, and papillary muscles, allowing blood to move around the enlarged septum to the aortic valve in the area that the mitral valve once occupied.
- 45. The primary complication of both procedures is dysrhythmia; additional complications as postoperative surgical complications such as pain, ineffective airway clearance, deep vein thrombosis, risk for infection, and delayed surgical recovery.
- 46. PREVENTION In many cases, you cant prevent cardiomyopathy. You can help reduce your chance of cardiomyopathy and other type of heart diseases by living a heart healthy lifestyle and making lifestyle choices such as:- Avoiding the use of alcohol or cocaine. Controlling high blood pressure,
- 47. high cholesterol and diabetes. Eating a healthy diet. Getting a regular exercise. Getting enough sleep. Reducing your stress.
- 48. SUMMARY Today we have seen regarding, Definition of cardiomyopathy Types of cardiomyopathy Causes, pathophysiology,signs and symptoms , risk factors of cardiomyopathy Complications of cardiomyopathy
- 49. Diagnostic tests Medical management Nursing management Surgical management Prevention
- 50. CONCLUSION Cardiomyopathy (CMP) constitutes a group of diseases that directly affect the structural or functional ability of the myocardium. In general , when someone refers to a cardiomyopathy they mean the three common types. Some people will use cardiomyopathy in reference to an ischemic cardiomyopathy, which implies that atherosclerotic coronary diseases has resulted in left ventricle systolic dysfunction.
- 51. This is technically Improper use of the term cardiomyopathy; however, it is much easier to say/ write than “ chronic systolic congestive heart failure from ischemic heart diseases.” Likewise, the term “non-ischemic cardiomyopathy” is frequently used when the ventricular systolic function is low from a non-ischemic cause) i.e (dailated cardiomyopathy).
- 52. BIBLIOGRAPHY 1. P.Hariprasath, “Textbook of Cardiovascular & Thoracic Nursing”, First Edition 2016, Jaypee Brothers Medical Publishers (P) Ltd, page no. 523- 532. 2. Javed Ansari, Davinder Kalir;”Text Book of Medical Surgical Nursing- I” Part A, Published by PV Books, 2015 edition, Pageno. 17 – 19.
- 53. 3. Suzanne C. Smelter, Brenda Bare, “Brunner and Suddarth’s Textbook of Medical Surgical Nursing”, 10th edition, published by Lippincott Williams and Wilkins, page no. 4. Janice L Hinkle, Kerry H Cheever,” Brunner and Suddarth’s Textbook of Medical Surgical Nursing”, volume 1, 13th edition, published by, Wolters Kluwer, New Delhi, page no.29-31.