
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Tibialis anterior muscle herniation in athletes
Similar to Tibialis anterior muscle herniation in athletes (20)
Recently uploaded
Recently uploaded (20)
Tibialis anterior muscle herniation in athletes
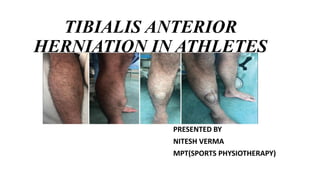
- 1. TIBIALIS ANTERIOR HERNIATION IN ATHLETES PRESENTED BY NITESH VERMA MPT(SPORTS PHYSIOTHERAPY)
- 2. Tibialis Anterior Muscle • Origin: Lateral condyle of tibia - Upper two third of lateral surface of tibial shaft and adjoining surface of interosseous membrane • Insertion: Inferiomedial surface of median cuneiform and adjoining part of base of first metatarsal bone • Action: In non-weight bearing position - Dorsiflexion of foot - Inversion of foot
- 3. Continue….. In weight bearing position - With Tibialis Anterior control eversion of foot and big component of foot pronation - Maintains medial longitudinal arch of foot • Nerve supply: Deep Peroneal nerve • Artery: Anterior Tibial artery
- 5. Tibialis Anterior Muscle Herniation • Muscle hernia was first described by Hugo Ihde in 1929 and first reported case in Kingdom of Bahrain • There are about 200 cases of muscle hernias described in literature • Hernia is defined as protrusion of tissue contained within a cavity through the wall of cavity that contains it • Muscle hernias are focal herniation of muscle tissue through a defect in its fascial sheath • Tibialis anterior muscle herniation is most common type of skeletal muscle herniation in lower limb
- 6. Continue….. • Other muscles are- Peroneus longus muscle and Rectus Femoris muscle • Muscle protrude through a defect in fascia into subcutaneous fat and present as a soft nodule • Characteristic presentation of hernia is local visible mass at the site of defect and more prominent in weight bearing position or resisted dorsiflexion of ankle joint • Presents in athletes, soldiers, mountain climbers and in professions requiring excessive strain on legs
- 7. EHL= Extensor hallucis longus EDL= Extensor digitorum longus FDL= Flexor digitorum longus FHL= Flexor hallucis longus PB= Peroneus brevis PL= Peroneus longus
- 8. Causes: • Trauma A. Penetrating trauma: Direct injury to the fascia B. Direct trauma: Closed fracture that cause fascial tear C. Indirect trauma: Force applied to the contracted muscle causing acute fascial tear • Constitutional hernia/Congenital hernia 1. Occur due to weakness in muscle fascia, after chronic stress
- 9. Continue…. 2. May involve the fascial tissue as a whole or only a localized site where blood vessels or nerves passes through the fascia 3. There are fenestrations in muscle compartments through which perforating veins enter 4. Due to chronic stress, fenestrations enlarge and eventually muscle hernias through these openings
- 10. Sign and Symptoms: • Asymptomatic • Localized swelling/Nodule • Dull pain at the site of swelling • Cramping • Pain decreased with rest • Numbness in the lateral portion • Decreased swelling in supine positon • Dorsiflexion weakness • Increased localized pain and swelling in Fencer’s lunge position
- 11. Differential Diagnosis: • Piezogenic pedal papules • Lipoma • Hematoma • Fibroma • Epidermoid cyst • Tumour • Varicose vein • Arteriovenous aneurysm
- 12. Confirmatory Diagnosis: Diagnostic Ultrasound Magnetic Resonance Imaging (MRI) Tibialis anterior muscle hernia : Diagnostic Ultrasound by Dr Maulik S Patel Tibialis anterior muscle hernia: a rare differential of a soft tissue tumour Arun et al 2015
- 13. Conservative Management: • Stage 1: Rest and avoid weight bearing Compression stockings/crepe bandage Isometric exercise for Tibialis anterior muscle • Stage 2: Concentric contraction of Tibialis anterior in weight bearing position • Stage 3: Eccentric exercises for Tibialis anterior muscle • Stage 4: Sports-specific Plyometric exercises
- 14. Surgical Management: • When conservative management fails then need to go for surgical treatment • Most commonly used surgical technique is direct closure of fascia defect by tightening the area (high chance of re-herniation) • This technique increases the intracompartmental pressure and later patient may develop anterior compartment syndrome • More successful and current surgical approach is longitudinal fasciotomy with or without a graft/synthetic mesh
- 15. Post operative Physiotherapy management • In small muscular hernia no specific post operative physiotherapy treatment required • But in large hernia post operative physiotherapy is important for patient to go back in particular sports
- 16. Continue…….. S.No. INTERVENTION POSITIONING PROCEDURE FREQUENCY 1. Short leg splint TP*: Standing PP** Supine/long sitting Ankle in moderate (5-10◦) plantarflexion 2 hours on and 1 hour off Remove during exercise and sleeping 2. Isometric exercise TP: Standing PP: Supine/long sitting Patient is asked to pull the foot towards self Hold for 5 seconds and repeat the exercise for 10 times x 2 sets, 3 times a day 3. Non weight-bearing walking with walker TP: Standing next to patient PP: Walker standing Patient is advised to walk without touching affected limb on the ground 6 minutes x 2 times a day
- 17. Continue….. 4. Concentric exercise TP: Standing towards foot end of patient PP: Supine with foot out of the couch This exercise is performed with help of a loop band. The therapist holds one side of the band and other end on patient’s forefoot. Patient is asked to pull the foot towards self Repeat the exercise 10 times x 3 sets, 3 times a day 5. Partial weight-bearing walking TP: Standing with patient PP: Standing with walker Patient is advised to place forefoot of affected limb on the ground during walking 6 minutes x 3 times a day 6. Full weight-bearing walking with walker TP: Standing with patient PP: Standing with walker Patient is asked to place both the feet on ground to initiate and progress walking 6 minutes x 3 times a day 7. Heel walking TP: Standing with patient PP: Standing Patient is instructed to walk on both heel 2 minutes x 3 times a day
- 18. Continue…. 8. Half squats (Bilateral) TP: Standing beside patient PP: Standing The patient is asked to perform half squat Hold for 30 seconds x 10 times x 3 sets, 2 times a day 9. Eccentric exercise TP: Standing towards foot end of patient PP: Supine/high sitting with foot out of the couch A loop band/theraband is overlapped over the forefoot of patient. One side is held by the patient and simultaneously is asked to push the forefoot towards the ground Repeat the exercise 10 times x 3 sets, 3 times a day TP*: Therapist Position PP**: Patient Position
- 19. THANK YOU