
Recommended
Recommended
More Related Content
Similar to venous anomalies Dr Nikhil.pptx
Similar to venous anomalies Dr Nikhil.pptx (20)
Recently uploaded
Recently uploaded (20)
venous anomalies Dr Nikhil.pptx
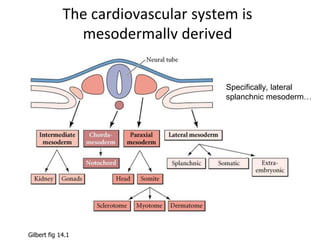
- 1. The cardiovascular system is mesodermally derived Specifically, lateral splanchnic mesoderm… Gilbert fig 14.1
- 2. The cardiogenic field is established in the mesoderm just after gastrulation (~18-19 days) and develops into a fully functional, multi-chambered heart by the 8th week angiogenic cell clusters (angioblasts/hemangioblasts) (right dorsal aorta) (right endocardial tube) blood islands (developing blood vessels) cardiogenic field pericardial cavity Langman’s fig 12-1
- 3. Fusing cardiac primordia “conotruncus” (outflow tract) future ventricles future atria septum transversum (liver & diaphragm primordium) 21 days 22 days Langman’s fig 12-7
- 4. Venous system development cardinal veins vitelline veins umbilical veins sinus venosus Langman’s fig 12-41
- 5. Vitelline and umbilical veins change during liver development • R hepatocardiac channel hepatic portion of IVC • R umbilical V regresses • proximal L umbilical V regresses • distal L umbilical V persists and then round ligament of the liver (ligamentum teres hepatis) • ductus venosus ligamentum venosum L vitelline V umbilical V sinus venosus cardinal V hepatic sinusoids duodenum duodenum yolk sac L hepatocardiac channel R hepatocardiac channel ductus venosus portal V superior mesenteric V splenic V hepatic portion of inferior vena cava hepatic V (R vitelline V) hepatic V 4 weeks 5 weeks 6 weeks 8 weeks
- 6. posterior cardinal veins anterior cardinal veins Systemic venous development Langman’s fig 12-41
- 7. Week four: SYMMETRY Umbilical Veins drain the chorion Vitelline Veins drain the yolk sac Cardinal Veins drain the body of the embryo. All three pairs of veins open to the right and left horn of the sinus venosus - at this stage the liver buds begin to develop from the ventral endodermal wall of the foregut - these cells invade mesenchymal tissue, called the septum transversum Umbilical Veins anterior cardinal veins Vitelline Veins
- 8. 5 – 8 weeks of gestation - liver cords growing into the septum transversum - interrupt the cranial portion of both vitelline (first) and umbilical veins (day 32) between the liver and the heart with an extensive vascular network – the hepatic sinusoids vitelline anastomoses
- 9. 5–8 weeks of development the asymmetric stage with intrahepatic umbilico–portal–ductus venosus anastomosis main portal vein duodenum left and right portal veins left ant. cardinal vein left ant. cardinal vein hepatocardiac segment of inferior v. cava 1. Left proximal vitelline vein disappears 2. Right proximal vitelline vein give rise to hepatocardiac segment of inferior v. cava 3. Distal sections of vitelline veins become portal vein 4. Other segments disappear Hepatic vein ductus venosus -joining of hepatic sinusoids -draining into IVC
- 10. Changes in umbilical veins at 5-8 weeks - changes of vitelline veins are accompanied by changes in umbilical veins 1. Entire right umbilical vein diappears 2. Cranial segment of left umbilical vein disappears left left right left Umbilical Vein becomes - dominant conduit of blood from placenta left umbilical vein 8th week - intrahepatic portion of the Vitelline Vein (left portal branch), forms an anastomosis between the intrahepatic segment of the left Umbilical Vein - and forms an anastomosis with ductus venosus main portal vein ductus venosus left umbilical vein hepatocardiac segment of inferior v. cava from right vitelline vein
- 11. Cardinal veins, subcardinal and supracardinal veins - anterior and posterior Cardinal Veins drain the embryo body, draining the cranial and caudal parts of the body - both veins empty into the Common Cardinal Veins – the third venous system entering the sinus venosus of the embryonic heart - as the embryo is growing in size, cardinal veins are supplemented by a range of bilateral longitudinal venous channels that anastomose with posterior cardinal system and with each other: subcardinal, supracardinal
- 13. Fate of Cardinal veins, subcardinal and supracardinal veins -left subcardinal vein -subcardinal anastomosis -left supracardinal vein -left posterior cardinal vein -iliac anastomosis of posteror cardinal veins -sub-supracardinal anastomosis (renal collar) 1. From the 5th week the posterior cardinal branches are obliterated - only the most caudal part persists giving rise to the common iliac vein - and most caudal segment of Inferior Vena Cava: sacral segment -left anterior cardinal vein -left common cardinal vein
- 14. Fate of Cardinal veins, subcardinal and supracardinal veins -left subcardinal vein -subcardinal anastomosis -left posterior cardinal vein -iliac anastomosis of posteror cardinal veins hepatocardiac segment of inferior v. cava (VV) 1. From the 5th week the posterior cardinal branches are obliterated - only the most caudal part persists giving rise to the common iliac vein - and most caudal segment of Inferior Vena Cava: sacral segment -left anterior cardinal vein -left common cardinal vein anastomosis between anterior cardinal veins
- 15. Fate of subcardinal veins, cardinal veins, and supracardinal veins hepatocardiac segment of inferior v. cava (VV) - subcardinal veins form in the ventromedial parts of mesonephric ridges (5-7 weeks) - become connected to postcardinal veins by a number of vessels - drainage of mesonephros By the 8th–9th week - the proximal left subcardinal vein obliterates and connects with the right branch: renal–hepatic (suprarenal) segment of the IVC - anastomosis between the subcardinal veins forms: proximal part of left renal vein -subcardinal anastomosis gonadal veins -sub-supracardinal anastomosis (renal segment)
- 16. Fate of supracardinal veins, cardinal veins, and subcardinal - supracardinal veins form dorsolateral to the aorta - supracardinal veins drain the thoracic wall and the iliac veins - inferior portion of the left supracardinal vein obliterates -and connects to the right subcardinal vein, - forming the sacrorenal (prerenal) segment of the IVC - superior segment of the supracardinal vein is divided: - into the left branch, called the hemiazygos vein, which forms a cross anastomosis to the right branch: called the azygos vein, which drains into the superior vena cava -sub-supracardinal anastomosis (renal segment) postrenal segment prerenal segment renal vein gonadal vein
- 17. Superior and inferior vena cava - proximal left anterior Cardinal Vein -regresses and disconnects from the sinus venosus -a shunt to the right anterior Cardinal Vein is formed: left brachiocephalic vein - right anterior Cardinal Vein is transformed into: right brachiocephalic vein - segment between the junction of the left and right brachiocephalic veins and the right atrium develops meanwhile into: Superior Vena Cava -right common cardinal vein -proximal part of right anterior cardinal vein – coronary sinus oblique vein -left sinus horn
- 18. Systemic venous development: shift to the right 7 weeks Adult L. brachiocephalic anastomosis What if the brachiocephalic anastomosis fails? Moore & Persaud
- 19. Double inferior vena cava Absent inferior vena cava Langman’s fig 12-45
- 20. Left superior vena cava Double superior vena cava viewed from behind Langman’s fig 12-46
- 21. ANOMALIES OF SYSTEMIC VENOUS SUPPLY • Anomalies of Caval Veins • Anomalous Connection with Normal Drainage 1. Superior caval vein a. Left superior caval vein to coronary sinus—with or without connecting vein
- 22. BILATERAL SUPERIOR VENAE CAVA WITH NORMAL DRAINAGE TO THE RIGHT ATRIUM
- 24. COURSE OF LSVC follows the course of the embryonic left cranial cardinal vein. It enters the pericardial cavity to the left of the left upper pulmonary veins, and runs posterior to the dome of the left atrium, having the mouth of the left atrial appendage to its left side. As it passes inferiorly, it accepts the hemiazygos vein and descends medially into the inferior atrioventricular groove. In nine-tenths of cases, the persistent left superior caval vein drains into the morphologically right atrium through an enlarged mouth of the coronary sinus
- 25. • THE SIZE OF THE LSVC VARIES • LEFT INNOMINATE VEIN MAY BE PRESENT IN 60% • THE LSVC STARTS AT THE JUNCTION OF THE LEFT JUGULAR AND LEFT SUBCLAVIAN VEINS • JOINS THE CORONARY SINUS IN THE POSTERIOR LEFT AV GROOVE
- 26. CLINICAL MANIFESTATIONS • PHYSIOLOGY IS USUALLY NORMAL AND NO CLINICAL MANIFESTATIONS • ENLARGEMENT OF THE CORONARY SINUS MAY INTERFERE WITH BLOOD FLOW FROM THE LA INTO THE LV • AN INCREASE IN THE MAGNITUDE OF THE LEFT TO RIGHT SHUNT AT THE ATRIAL LEVEL WAS FOUND IN PATIENTS WITH SECUNDUM ASD PERSISTENT LSVC AND DILATED CORONARY SINUS
- 27. • CHEST X-RAY : SHADOW ALONG THE LEFT UPPER BORDER OF THE MEDIASTINUM
- 28. BILATERAL SVC WITH AN UNROOFED CORONARY SINUS • COMMON WALL BETWEEN THE LA AND CORONARY SINUS IS ABSENT • PERSISTENT LSVC DRAINS INTO THE LEFT ATRIUM • IN PATIENTS WITH A NORMAL INTER ATRIAL SEPTUM, THE ORIFICE OF THE UNROOFED CORONARY SINUS WILL FUNCTION AS AN INTERATRIAL COMMUNICATION
- 29. CLINICAL MANIFESTATIONS • MOST PATIENTS HAVE A LARGE CORONARY SINUS OSTIUM THAT FUNCTIONS AS AN INTERATRIAL COMMUNICATION (RAGHIB SYNDROME) • IN MOST PATIENTS, ARTERIAL OXYGEN SATURATION RANGES BETWEEN 85-95% • THEY ARE AT RISK OF PARADOXICAL EMBOLI, BRAIN ABSCESS, STROKE • WHEN RIGHT ATRIAL OUTFLOW STENOSIS OR ATRESIA COEXISTS WITH A PERSISTENT LSVC TO AN UNROOFED CORONARY SINUS, THE SHUNT IS FROM RIGHT TO LEFT
- 30. • REPAIR IS DONE TO AVOID COMPLICATIONS OF CYANOSIS • IF THE LSVC OS RELATIVELY SMALL AND THERE IS AN ADEQUATE SIZED LEFT INNOMINATE VEIN, THE LSVC CAN BE LIGATED AND THE INTERATRIAL COMMUNICATION CLOSED. • IN THE ABSENCE OF AN ADEQUATE SIZED BRIDGING LEFT INNOMINATE VEIN, THE CORONARY SINUS IS REROOFED.
- 31. ABSENCE OF RIGHT SUPERIOR CAVAL VEIN • The anomaly results from involution of the right, instead of the left, superior cardinal vein during embryonic life. It is known to exist both as an isolated anomaly and in association with other cardiac malformations. Abnormalities of rhythm are common, more so with coexisting cardiac malformations, and are more pronounced in older patients • RHYTHM DISTURBANCES INCLUDE: AV block, SA node dysfunction, VT, LBBB And RBBB, SVT
- 32. Issues that make diagnosis important are • Implantation of transvenous pacemaker • placement of a pulmonary artery catheter for intraoperative or postoperative monitoring without the use of flouroscopy • systemic venous cannulation for ECMO, CPB
- 33. Absent Bilaterally Superior Caval Veins On rare occasions, both superior caval veins can be absent. The blood from the head and arms drains to the inferior caval vein via the azygos or hemiazygos systems. Although the exact morphogenesis remains unclear, we presume that this anomaly results from failure of development of the superior cardinal venous system. Since the drainage of blood remains unobstructed, it remains clinically silent, as has been the case in most reported examples, coming to attention only during pacemaker implantation or central line insertion
- 34. INFERIOR CAVAL VEIN A. Absence of the Hepatic Segment of Inferior Caval Vein With Azygos Continuation This is the most common anomaly involving the inferior caval vein. It exists because of the absence of the infrahepatic portion of the inferior caval vein (INTERRUPTED IVC). The blood from the lower part of the body reaches either the left or right superior caval vein via the dilated azygos venous system Hepatic veins drain blood from Liver to Morphological RA occurs dur to Abnormal development of right subcardinal vein which fails to anastomose to right vitelline vein.
- 35. • Supracardinal venous system normally forms Azygous vein which provides drainage to developing superior caval vein • INCIDENCE: 0.6% • It is most relevant in the setting of patients having functionally univentricular hearts who are undergoing construction of a cavopulmonary connection. The mere connection of the superior caval vein to the pulmonary arteries in this setting is equivalent to a near total cavopulmonary connection. This is so-called Kawashima repair
- 36. Anomalous Systemic Venous Connection With Anomalous Drainage • SYSTEMIC VEIN DRAIN - MORPHOLOGICALLY LA • DIRECT DRAINAGE - BLOOD AWAY FROM PULMONARY CIRCULATION ( DECREASES EFFECTIVE PULMONARY FLOW) • RISK OD PARADOXICAL EMBOLISATION AND STROKE • ARTERIAL DESATURATION DISPROPORTIONATE TO CO-EXISTING CARDIAC MALFORMATION
- 37. LSVC TO LA • The left superior caval vein can rarely communicate directly and anomalously to the left atrium. In most of these instances, the communication is through a combined deficiency of the adjacent walls of the left atrium and coronary sinus. The spectrum of fenestration of the coronary sinus is also described as unroofing of coronary sinus • Unroofed coronary sinus almost always is associated with a persistent LSVC • A CS defect without an associated LSVC, and the physiology is same as in ASD
- 38. RIGHT SVC DRAINING INTO LA • IT REPRESENTS A SINUS VENOSUS DEFECT OF THE SVC TYPE IN ASSO. WITH ATRESIA OF THE RIGHT SVC ORIFICE RESULTS FROM DEF. OF COMMON WALL BETWEEN SVC AND RUPV THIS DEFECTS UNROOF THE RUPV AND ITS BRANCHES INTO RIGHT SVC THE UNROOFED RUPV THEN DRAINS INTO SVC AND ITS LA ORIFICE BECOMS INTERATRIAL COMMUNICATION
- 39. CLINICAL MANIFESTATIONS OF R-SVC IN LA • CYANOSIS • SYMPTOMS MAY NOT DEVELOP UNTIL LATE CHILDHOOD OR ADOLSCENCE • THE RISKS OF RT TO LT SHUNT SEQUELAE INCREASE WITH AGE
- 40. • TREATMENT • THE RIGHT SVC FLOW IS SURGICALLY DIVERTED INTO THE RA • IN THE PAST THIS WAS DONE BY CREATING AN ASD AND REDIRECTING SVC FLOW INTO RA AND PULMONARY BLOOD INTO LA • PREFERRED SURGICAL APPROACH IS TRANSECTION OF THE RIGHT SVC ABOVE THE ENTRANCE OF THE RUPV AND ANASTOMOSIS OF THE TRANSECTED CAVAL END TO THE RA APPENDAGE
- 41. BILATERAL INFERIOR VENAE CAVA • BILATERAL SUPRAHEPATIC IVCs (i.e. A NORMAL IVC AND A CONTRALATERAL HEPATIC VEIN) A FREQUENT FINDING IN CASES OF VISCERAL HETEROTAXY WITH ASPLENIA • B/L SUPRAHEPATIC IVCs ALSO CAN OCCUR RARELY IN PATIENTS WITH A NORMAL VISCERAL SITUS • THE LEFT SIDED HEPATIC VEIN IN THOSE CASES CASES DRAINS INTO A NORMAL CS
- 42. INFERIOR VENA CAVA DRAINAGE TO THE LA • DURING FETAL LIFE ABOUT HALF OF THE UVC BLOOD THAT ENTERS THE RA IS DIRECTED TOWARDS THE LA WITH HELP OF TWO VENOUS VALVES, THE EUSTACHIAN VALVE ANDD VALVE OF THE FORAMEN OVALE • A LEFT ATRIAL IVC ALSO OCCUR IN CASES IN WHICH ALL THE SYSTEMIC AND ALL THE PVs DRAINED INTO THE LEFT SIDED ATRIUM
- 43. CLINICAL MANIFESTATIONS • PARTIAL OR COMPLETE DRAINAGE OF THE IVC NTO THJE LEFT ATRIUIM RESULTS IN CYANOSIS • THE CLINICAL MANIFESTATIONS ARE THE RESULT OF RIGHT TO LEFT SHUNTING, INCLUDING POLYCYTHEMIA, BRAIN ABSCESS, AND PARADOXICAL EMBOLI • TREATMENT : IVC BLOOD IS SURGICALLY REDIRECTED INTO THE RIGHT ATRIUM
- 44. TOTALLY ANOMALOUS SYSTEMIC VENOUS CONNECTION • CONNECTION OF ALL SYSTEMIC VEINS, ALONG WITH THE PVs, TO MORPHOLOGIC LA --> RARE, PARTICULARLY WHEN ATRIAL ARRANGEMENT IS USUAL • WHEN PRESENT AS ISOLATED ANOMALY LEFT TO RIGHT SHUNT (ASD/VSD/PDA) PROVIDES BLOOD TO LUNGS--> DETERMINES SPO2 • AMOUNT OF LEFT TO RIGHT SHUNT GOVERNS GROWTH OF RA/RV • SMALL SHUNTS-HYPOPLASIA OF RIGHT CHAMBERS- INTENSE CYANOSIS
- 45. • LARGE SHUNT: GOOD OXYGENATION, GROWTH OF RV, PERMITTING COMPLETE SURGICAL REPAIR • PRESENCE OF CYANOSIS DESPITE OF L--> R SHUNT ACROSS ASD, HYPOPLASTIC RV, CONCORDAND AV + VA CONNECTIONS --> ALMOST DIAGNOSTIC OF TASVC • DIAGNOSIS IS MISINTERPRETED AS SINGLE VENTRICULAR PHYSIOLOGY • ONLY 1 CAVAL VEIN GENERALLY SVC MAYBE CORRECTLY IDENTIFIED BECAUSE SALINE CONTRAST ECHO IS PERFORMED FROM UPPER LIMB
- 46. FINDINGS • INTENSE CYANOSIS, CLUBBING • JVP: NOT ELEVATED • NO CARDIOMEGALY, LIVER NORMAL SIZE • ECG: POOR RV FORCES • ECHO: AV+VA CONCORDANCE, ALL PVS TO LA, DRAINAGE OF CAVAL VEINS NOT CLEARLY VISUALIZED USUALLY, HYPOPLASTIC RA/RV, DILATED LA/LV • AGITATED SALINE INJECTED IN RIGHT ARM: IMMEDIATE + INTENSE FILLING OF LA FOLLOWED BT RA • CARDIAC CATH: CONTRAST INJECTION IN CAVAL VEINS CONFIRMS SVC+IVC+HEPATIC VEINS CONN. TO LA, SWAN GANZ CATHETER INSERTED THROUGH RFA>AO VALVE>LV>MV>LA>ASD>RA
- 49. ANOMALIES OF DUCTUS VENOSUS • 1. ANOMALOUS TERMINATION OF THE UMBILICAL VEINS AND ABSENT DUCTUS VENOSUS • 2. POSTNATAL PERSISTENCE OF THE DUCTUS VENOSUS • 3. PERSISTENT VALVES OF THE SINUS VENOSUS
- 50. • 1. ANOMALOUS TERMINATION OF THE UMBILICAL VEINS AND ABSENT DUCTUS VENOSUS: • PERSISTENT LEFT UMBILICAL VEIN TERMINATES DIRECTLY INTO THE CS, BY WAY OF THE LEFT PORTAL VEIN OR INTO THE ILIAC VEIN • PERSISTENT RIGHT UMBILICAL VEIN TERMINATES DIRECTLY INTO THE RA, INTO THE IVC, INTO THE RIGHT PORTAL VEIN AND INTO RIGHT SVC
- 51. • CLINICAL MANIFESTATIONS: • USUALLY DO NOT PRODUCE SYMPTOMS • INTRAUTERINE OBSTRUCTION OF THE UMBILICAL VEIN FLOW AND POSTNATAL INTESTINAL OBSTRUCTIONS SECONDARY TO THE ANOMALOUS TERMINATION OF THE UMBILICAL VEIN MAY OCCUR
- 52. POSTNATAL PERSISTENCE OF THE DUCTUS VENOSUS • CONGENITAL POSTNATAL PERSISTENCE OF THE DUCTUS VENOSUS BECAUSE THE SHUNT WAS AWAY FROM THE PORTAL VENOUS SEPTUM PROXIMALLUY TO THE DISTAL HEPATIC VEINS OR IVC DISTALLY • THESE INTRAHEPATIC PORTO-SYSTEMIC SHUNTS ARE DUE TO ABNORMAL PERSISTENCE OF ELEMENTS OF THE OMPAHALOMESENTRIC SYSTEM • THREE OF THE TEN CASES REPORTED RESULTED IN PORTO-SYSTEMIC ENCELOPATHY
- 53. • DIAGNOSIS: ULTRASOUND OR CT DEMONSATRATES A LARGE TORTOUS VESSEL ORIGINATING FROM THE PORTAL VEIN THAT CONNECTED TO THE HEPATIC VEIN OR IVC • TREATMENT: IN THE ABSENCE OF ENCEPHALOPATHY, T/T MAY NOT BE INDICATED. IF LIGATION OF THE DUCTUS VENOSUS IS CONTEMPLATED ONE SHOULF ESTABLISH THE INTERGRITY OF THE PORTAL SYSTEM. IF IT IS NOT INTACT, LIGATION COULD LEAD TO MESENTRIC VENOUS CONGESTION > BOWEL ISCHEMIA
- 54. EXTRAHEPATIC POSTOSYSTEMIC SHUNT ( ABERNETHY MALFORMATION) • Uncommonly, the blood from the splanchnic circulation reaches the IVC via abnormal vascular communications. These anomalous portosystemic shunts (Abernethy malformation) • Have hemodynamic and clinical implications comparable to those produced by persistent patency of the venous duct. However, the communication is located outside the liver. • Well known to exist with hypoplasia of intrahepatic portal venous system. The variant with absent portal vein is more common in females. If suspected, the diagnosis can be easily made by ultrasound and or computed tomographic angiography. While liver transplantation is the only treatment available when the intrahepatic portal veins are absent, closure or ligation of the shunt can be performed in the setting of hypoplasia
- 55. ANOMALIES OF THE CORONARY SINUS • CORONARY SINSUS DEFECT AND UNROOFED CS • CORONARY SINUS ORIFICE ATRESIA • UNROOFED CORONARY SINNUS ALMOST ALWAYS IS ASSOCIATED WITH A PERSISTENR LSVC • A CS DEFECT WITHOUT AN ASSOCIATED LSVC, AND THE PHYSIOLOGY IS THE SAME AS IN ASD
- 56. CORONARY SINUS ORIFICE ATRESIA • INCIDENCE IS RARE • THE CS IS USUALLY WELL FORMED, THE ORIFICE IS COVERED BY A THIN MEMBRANE LIKE TISSUE • ALTERNATIVE EXIT FOR CORONARY VENOUS BLOOD RETURN- – A SMALL LSVC, LARGE THEBASIAN VEIN – CS SEPTAL DEFECT, CONNECTION WITH THE IVC IN ONE CASE
- 57. • It is also possible for the thebesian valve to persist and to produce atresia of the orifice of the sinus. In this situation, coronary venous drainage will be to a persistent left superior caval vein, which may well be relatively hypoplastic. Intraoperative ligation of the caval vein in this setting was described as producing coronary ischemia and death. In some of these cases with atresia of the orifice of coronary sinus, an associated fenestration in the walls of the sinus permits drainage of coronary venous blood to the left atrium.
Editor's Notes
- 2