
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Complications of som
Similar to Complications of som (20)
Recently uploaded
Recently uploaded (20)
Complications of som
- 1. INRACRANIAL COMPLICATIONS OF OTITIS MEDIA DR.NEENA KARUNA KARAN MMCH
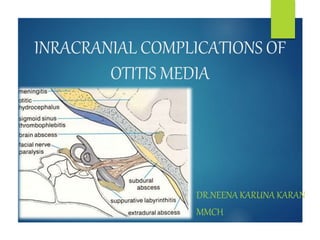
- 2. COMPLICATIONS OF OTITIS MEDIA INTRA TEMPORAL • Mastoiditis • Petrositis • Facial paralysis • Labyrinthitis INTRA CRANIAL • Extra dural abscess • Subdural abscess • Meningitis • Otogenic brain abscess • Lat. Sinus thrombophlebitis • Otitic hydrocephalus
- 3. OTOGENIC BRAIN ABSCESS In adults Usually follows CSOM with cholesteatoma In children As a result of acute otitis media
- 4. ROUTES OF INFECTION • Direct extension of ME infection through tegmen • Retrograde thrombophlebitis Cerebral abscess • Direct extension through Trautmann’s triangle • Retrograde thrombophlebitis Cerebellar abscess
- 7. Bacteriology AEROBIC • Staphylococci • S.pneumoniae • S.haemolytics • E.coli • P.aeruginosa ANAEROBIC • Peptostreptococcus • Bacteroid fragilis
- 8. PATHOLOGY STAGE OF INVASION • Head ache ,low grade fever STAGE OF LOCALIZATION • No symptoms • Localize the pus by formation of capsule STAGE OF ENLARGEMENT • Abscess began to enlarge • Zone of edema -aggravation of symptoms STAGE OF TERMINATION Ruptures into ventricle /sub arachnoid space fatal meningitis
- 10. CLINICAL FEATURES THOSE DUE TO RAISED INTRACRANIAL TENSION Headache-worse in the morning Nausea & vomiting Level of conciousness lethargy drowsiness confusion stupor coma Papilloedema Slow pulse & subnormal temperature
- 11. LOCALIZING FEATURES Temporal lobe abscess Nominal aphasia Homonymous hemianopia: pressure on optic radiation Contralateral motor paralysis: upward spread- face arm leg Inward spread - leg arm face Epileptic fits Pupillary changes & oculomotor palsy
- 12. Cerebellar abscess Headache Spontaneous nystagmus Ipsilateral hypotonia & weakness Past pointing & intention tremor Dysdiadochokinesia
- 13. INVESTIGATIONS Skull X-rays CT scan o site &size of the lesion o reveals associated complications X -ray mastoids or CT scan of temporal bone Lumbar puncture : CSF shows- rise in pressure protein content WBC Count polymorphs/lymphocytes
- 14. TREATMENT MEDICAL High doses of antibiotics parenterally o Mixed infections: o chloramphenicol+ 3rd gen.cephalosporins o Bacteroides fragilis : metronidazole o Pseudomonas/proteus : aminoglycosides ICT--Dexamethasone 4 mg iv 6 hrly / mannitol 20% in doses of .5g/kg body wt Discharge from ear-Suction clearence & topical ear drops
- 15. NEUROSURGICAL Abscess can be approached in following ways : Repeated aspiration through a burr hole Excision of abscess Open incision of the abscess &evacuation of pus
- 16. OTOLOGIC AOM Resolve with antibiotics given for abscess COM Radical mastoidectomy
- 17. LATERALSINUS THROMBOPHLEBITIS SIGMOID SINUS THROMBOSIS It is an inflammation of inner wall of lateral venous sinus with formation of an intrasinus thrombus.
- 18. PATHOLOGY 1.Formation of perisinus abscess 2.Endophlebitis & mural thrombus formation 3.Obliteration of sinus lumen & intrasinus abscess 4.Extension of thrombus
- 22. BACTERIOLOGY • S.haemolyticus • Pneumococcus • Staphylococcus Acute infections • Bacillus proteus • E.coli • P.pyocyaneus Chronic infections
- 23. CLINICAL FEATURES Hectic picket fence type of fever with rigors
- 24. Head ache Progressive anaemia & emaciation Griesinger’s sign - due to thrombosis of mastoid emissary vein
- 25. Papilloedema its presence depends on obstruction to venous return. Tobey –Ayre’s test Record CSF pressure by manometer
- 27. Crowe -beck test Pressure on jugular vein of healthy side engorgement of retinal veins & supra orbital veins Tenderness along jugular vein
- 28. INVESTIGATIONS Blood smear : to rule out malaria Blood culture : to find out causative organisms CSF examination : shows rise in pressure X ray mastoid : clouding of cells - acute mastoiditis destruction of bone – cholesteatoma
- 29. Imaging studies Culture & sensitivity of ear swab
- 30. COMPLICATIONS Septicaemia & pyaemic abscesses Meningitis & subdural abscess Cerebellar abscess Thrombosis of jugular bulb & jugular vein Cavernous sinus thrombosis Otitic hydrocephalus
- 31. TREATMENT IV antibacterial therapy: should be continued at least for a week after the operation Mastoidectomy & exposure of sinus: complete cortical/modified radical mastoidectomy Sinus bony plate is removed to expose the dura & drain the perisinus abscess
- 34. Ligation of internal jugular vein Anticoagulant therapy: used when thrombosis is extending to cavernous sinus Supportive treatment: Repeated blood transfusions
- 35. OTITIC HYDROCEPHALUS Characterised by raised intra cranial pressure with normal CSF findings
- 36. MECHANISM middle ear infection lateral sinus thrombosis Obstruction to thrombosis exends to venous return sup.sagittal sinus impede CSF absorbption by arachanoid villi raised intra cranial tension
- 37. CLINICAL FEATURES Symptoms Severe head ache Diplopia Blurring of vision
- 38. Signs Papilloedema Nystagmus Lumbar puncture CSF pr exceeds 300 mm H2O
- 39. TREATMENT to reduce CSF pr … achieved by Acetazolamide Corticosteroids Repeated lumbar puncture Placement of lumbar drain Lumbo peritoneal shunt Middle ear infection Antibiotic therapy Mastoid exploration