Defebrilation
•
6 likes•1,174 views

This document discusses defibrillation, which is a treatment used to restore normal heart rhythm in patients experiencing ventricular fibrillation or pulseless ventricular tachycardia. It defines defibrillation and describes the different types of defibrillators, including manual external defibrillators, automated external defibrillators, implantable cardioverter defibrillators, and wearable cardiac defibrillators. It also covers how defibrillation works, the precautions that must be taken with the procedure, and the risks involved.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Defebrilation
Similar to Defebrilation (20)
More from Naveen Pareek
Recently uploaded
Recently uploaded (20)
Defebrilation
- 2. OBJECTIVE:-
- 3. Definition:-
- 4. To eradicate life-threatening ventricular fibrillation or pulseless ventricular tachycardia. To restore cardiac output lost due to dysrhythmias and reestablish tissue perfusion and oxygenation.
- 5. The exact mechanism of defibrillation is not well understood. One theory is that successful defibrillation affects a critical mass of the heart, resulting in insufficient remaining heart muscle to continue the arrhythmia. Recent mathematical models of defibrillation are providing new insight into how cardiac tissue responds to a strong electrical shock. Fibrillations cause the heart to stop pumping blood, leading to brain damage. Defibrillators deliver a brief electric shock to the heart, which enables the heart's natural pacemaker to regain control and establish a normal heart rhythm.
- 6. Defibrillator Conductive medium- defibrillator pads Cardiac monitor with recorder Emergency cart and medications Emergency pacing equipment
- 7. Defibrillator is a device that gives a high energy electric shock to the heart of someone who is in cardiac arrest.
- 8. Manual external defibrillator Manual internal defibrillator Automated external defibrillator Implantable cardioverter defibrillator Wearable cardiac defibrillator
- 9. 1. Manual external defibrillator:- These defibrillators require more experience and training to effectively handle them. Hence, they are only common in hospitals and a few ambulances where capable hands are present. In conjunction with an ECG, the trained provider determines the cardiac rhythm and then manually determines the voltage and timing of the shock—through external paddles—to the patient’s chest.
- 10. 2. Manual internal defibrillator:-The manual internal defibrillators use internal paddles to send the electric shock directly to the heart. They are used on open chests, so they are only common in the operating room. It was invented after 1959. 3. Automated external defibrillator:-These are defibrillators that use computer technology, thereby making it easy to analyze the heart’s rhythm and effectively determine if the rhythm is shockable. They can be found in medical facilities, government offices, airports, hotels, sports stadiums, and schools.
- 11. 4. Implantable cardioverter defibrillator:-Another name for this is automatic internal cardiac defibrillator (AICD). They constantly monitor the patient’s heart, similar to a pacemaker, and can detect ventricular fibrillation, ventricular tachycardia, supraventricular tachycardia, and atrial fibrillation. When an abnormal rhythm is detected, the device automatically determines the voltage of the shock to restore cardiac function. 5. Wearable cardiac defibrillator:-is a portable external defibrillator generally indicated for patients who are not in an immediate need for an AICD. This device is capable of monitoring the patient 24-hours-a-day. It is only functional when it is worn and sends a shock to the heart whenever it is needed.
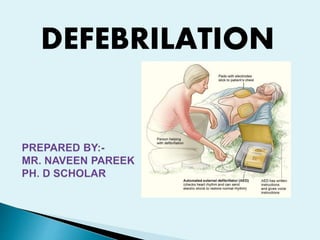
- 12. Resuscitation electrodes are placed according to one of two schemes. The anterior-posterior scheme is the preferred scheme for long-term electrode placement. One electrode is placed over the left precordium (the lower part of the chest, in front of the heart). The other electrode is placed on the back, behind the heart in the region between the scapula. This placement is preferred because it is best for non-invasive pacing. The anterior-apex scheme can be used when the anterior-posterior scheme is inconvenient or unnecessary. In this scheme, the anterior electrode is placed on the right, below the clavicle. The apex electrode is applied to the left side of the patient, just below and to the left of the pectoral muscle. This scheme works well for defibrillation and cardio version, as well as for monitoring an ECG.
- 14. Precautions:- 1. should not be performed on a patient who has a pulse or is alert, as this could cause a lethal heart rhythm disturbance or cardiac arrest. 2. paddles used in the procedure should not be placed on a woman's breasts or over an internal pacemaker. 3. During external defibrillation, the paddles are placed on the patient's chest with a conducting gel ensuring good contact with the skin. 4. Direct contact with the patient is discontinued by all caregivers. 5. The patient's pulse and/or electrocardiogram are continually monitored when defibrillation is not in progress. 6. Defibrillation continues until the patient's condition stabilizes or the procedure is ordered to be discontinued. 7. Medications to treat possible causes of the abnormal heart rhythm may be administered.
- 15. patient is found in cardiac distress, without a pulse and non-responsive, and help is summoned, cardiopulmonary resuscitation is begun and continued until the caregivers arrive and are able to provide defibrillation. Electrocardiogram leads are attached to the patient chest. Gel or paste is applied to the defibrillator paddles, or two gel pads are placed on the patient's chest. The caregivers verify lack of a pulse while visualizing the electrocardiogram, assure contact with the patient is discontinued, and deliver the electrical charge.
- 16. 1. Vital signs are monitored with a cardiac monitor 2. 12 lead electrocardiogram, 3. A chest x-ray 4. Cardiac catheterization Risks:- 1. Skin burns from the defibrillator paddles. 2. injury to the heart muscle 3. abnormal heart rhythms 4. blood clots.
- 18. Thank you