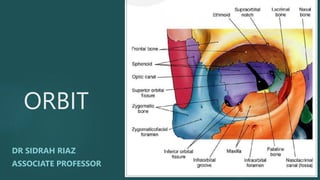
7. ROOF
Orbital plate of frontal bone
Lesser wing of sphenoid
Frontal bone
LATERAL WALL/ strongest wall
Frontal process of zygomatic
orbital surface of greater wing of sphenoid posteriorly
Thickest wall of the orbit
Separated posteriorly by superior orbital fissure ORBIT
8.
9. FLOOR
Orbital plate of maxilla
Zygomatic bone
Orbital process of palatine bone,
It roofs maxillary sinus, Its thin and is
most commonly fractured.
MEDIAL WALL / weakest wall
Orbital plate of ethmoid bone(lamina
papyracia)
lacrimal bone, At the apex – body of
sphenoid, Lacrimal bone contains fossa
for nasolacrimal sac
10. Proptosis
Proptosis refers to
forward protrusion of
the globe with respect
to the orbit. There are
many causes of
proptosis which can be
divided according to
location and it is worth
remembering that it is
not just orbital disease
processes that cause
proptosis
11. Proptosis causes
Remember the main causes of Proptosis using the mnemonic THE-I .
THE I (I~eye)
Tumor (Rhabdomyosarcoma, Retinoblastoma)
Hemorrhage (traumatic posterior orbital hematoma)
Endocrinopathy (Graves’ disease/TED)
Infection (pre septal cellulitis, orbital cellulitis,
Cavernous sinus thrombosis, orbital abscess)
14. ORBITAL SEPTUM
The orbital septum (palpebral
ligament) is a membranous sheet
that acts as the anterior boundary
of the orbit. It extends from the
orbital rims to the eyelids. It forms
the fibrous portion of the eyelids.
16. Pre septal cellulitis
Preseptal cellulitis is an inflammation and infection of the eyelid (also
of the periorbital soft tissues), anterior to orbital septum, characterized
by acute eyelid erythema and edema
It may result from the spread of the upper respiratory tract infections,
external eye infections (Stye), or eyelid trauma (laceration)
Patients with periorbital edema, erythema and increase in local
hyperemia but without proptosis, ophthalmoplegia and visual
impairment
Treatment: Antibiotics, Analdesics, Drainage of abscess
18. Clinical features
Impaired vision or sudden vision loss, RAPD POSITIVE
Pain, restricted ocular movement/ ophthalmoplegia
A red, swollen eyelid, chemosis
Proptosis
Discharge from the infected eye
Fever
Fatigue
Loss of appetite
Headache
19. Causes
The main cause of orbital cellulitis is sinusitis, which is an infection of
the sinuses, up to 86–98 % people with orbital cellulitis also have
sinusitis. Without treatment, sinus infections can spread to the fat and
muscle surrounding the eye socket
Bacteria such as the Staphylococcus aureus and Streptococci species
are the most common
An injury to the eye that penetrates the orbital septum
Complications of eye surgery
20. Indications for imaging
Eyelid edema that makes a complete examination impossible
Presence of CNS involvement (i.e seizures, focal neurologic deficits, or
altered mental status)
Deteriorated visual acuity or color vision
Proptosis
Ophthalmoplegia
Clinical worsening or no improvement after hours
23. Complications of orbital cellulitis
Intracranial extension of infection (i.e subdural empyema,
intracerebral abscess, extradural abscess and meningitis)
Cavernous venous sinus thrombosis
Septic emboli of the optic nerve
Optic nerve ischemia (due to compression) may result in
visual loss
26. Proptosis and
exophthalmos
Exophthalmos also describes forward
protrusion of the globe
Proptosis and exophthalmos are often used
interchangeably
Exophthalmos used to refer to severe (>18
mm) proptosis
Exophthalmos used to refer to endocrine-
related proptosis
Enophthalmos is the opposite,
displacement of the globe posteriorly
31. Pathophysiology
Infiltration of connective
tissue with mononuclear
cells (lymphocytes,
macrophages , plasma
cells)
Activation of CD4+ and
CD8+ T-cells and
integration with B cells,
plasmas cells and
macrophages.
Release of pro-
inflammatory
cytokines.
Accumulation of GAG in
the EOM and fat.
CD34 + fibrocytes
key in the
pathogenesis
Antigen in orbit :
Thyroglobulin
TSHR is found on
thyroid follicles and
orbital fibroblasts
32.
33.
34.
35.
36. Treatment of TED
Quit smoking
Medical Management of Hyperthyroidism• Anti-thyroid drugs :
Thinoamides (PTU), Carbimazole, Methimazole • Need 6-8 weeks to
achieve euthyroid state.
Side effects : Skin rash , urticarial , arthralgia , Fever
Corticosteroids • Intravenous , Oral , Topical
• IV pulse for Moderate to severe TED : 71% respond to IV steroid
• IV steroids for compressive ON
37. Orbital Radiation
• Mechanism : lymphocyte sterilization, destruction of tissue monocytes • 20 Gy in 10 divided
sessions over 2 weeks • More suited for patients > 35 years of age • Contra-indicated in pre-
existing retinopathy (diabetes , hypertensive)
Rituximab (for steroid resistant cases)
• it Targets CD20 • CD20 is expressed on more than 95% of B cells and plasma cells
• RTX depletes 95% of mature B cells , blocks Ab production , and decrease inflammatory
cytokine release
Botulinum Toxin / for proptosis
• Neurotoxin , inhibits acetylcholine release • For upper lid retraction (transconjunctival ,
transcutaneous route) • Effect on Muller’s muscle and LPS
• Side effects of Botox : bruising , ptosis and diplopia
Orbital Decompression for TED
• 2 wall or 3 wall • Decompression usually in stable phase of disease.
Squint surgery: later on/inactive disease
38.
39. Blow out fracture
The term Blow-out fracture
refers specifically to the
fracture of an orbital wall in the
presence of an intact orbital
rim
Mc Kenzie (1844) describe floor
fracture Smith and Converse
(1956) blow out fracture
40.
41. Clinical
features
External sign: Lid edema, subcutaneous or orbital emphysema
Ecchymosis
Subconjunctival hemorrhage
Enophthalmos
Inferior floor fracture; Diplopia due to IR entrapment
Infraorbital nerve hypesthesia (gum, side of nose)
Ocular Motility defects
42.
43. Evaluation
Visual acuity Pupil
intraocular
pressure
Biomicroscopy
and fundus
Check sensation
on
face(infraorbital
Nerve)
Ocular motility
test, Diplopia
chart & visual
fields
Photographs as
documentation
for patients to
appreciate
Force duction
test paretic and
restrictive
motility patterns
Radiology: X ray
, CT scans
44. Treatment of BOF
Conservative approach
Urgent surgical treatment
Early repair Indication
1. Symptomatic persistent diplopia with positive
force ductions.
2. CT evidence of orbital tissue or muscle
entrapment
3. No clinical improvement over 1 -2 weeks
4. Enophthalmos of 3 mm or more, globe ptosis,
floor defect > 50%
45. Conservative/ observation: if minimal diplopia with good motility, no
CT evidence of tissue entrapment, absence enophthalmos or globe
ptosis (give NSAIDs, antibiotics)
Surgical Repair: within 7 -10 days to allow swelling and hemorrhage to
subside , patient advised not to blow nose
Anesthesia: General (GA)
Approach: Transantral or transconjunctival via orbital rim, periosteum
elevated off the orbital floor until the fracture site is identified,
entrapped tissue is freed carefully and elevated from the defect insert
material for floor reconstruction