
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Vestibular schwanoma
Similar to Vestibular schwanoma (20)
More from MD Sayad Zaman
Recently uploaded
Recently uploaded (20)
Vestibular schwanoma
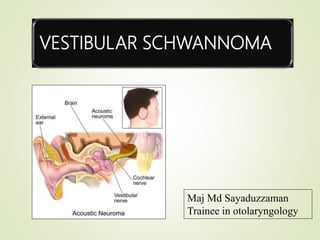
- 1. VESTIBULAR SCHWANNOMA Maj Md Sayaduzzaman Trainee in otolaryngology
- 2. vestibular schwannoma (VS) is an encapsulated benign tumour arising from abnormally proliferative schwann cells. The commonest nerve of origin is the superior vestibular nerve, followed by the inferior vestibular and then rarely, the cochlear nerve Acoustic neuroma represents 8% of all intracranial tumours and 80% of cerebellopontine angle tumours. The medial portions of the cranial nerves are covered with glial stroma. VS originate at the junction of the glial and Schwann cells, which for the vestibular nerve is usually within the internal auditory meatus vestibular schwannoma
- 3. CEREBELLOPONTINE ANGLE (CPA) CPA – Irregularly shaped potential space in the posterior fossa of the brain Boundary- Anteriolaterally – Petrous part of temporal bone Posterior – Cerebellum Superior – Pons Cerebellar peduncles Inferior – Cerebellar tonsils Medial – Lateral surface of the brainstem
- 4. Content of CPA CSF Cranial nerves and their associated vessels Superior:5th cranial nerve. 7th and 8th nerve Inferior : 9th,10th,11th nerves Anterior inferior cerebellar artery Superior petrosal veins
- 5. EPIDEMIOLOGY Both sexes are equally affected Age presentation is common between the ages of 40 and 60 Majority of these tumours are unilateral, and bilateral (5%) are seen in neurofibromatosis type 2 (NF2) Mean growth rate – 1.1 mm /year
- 6. Tumor pathogenesis Owing to mutations in the gene for the tumor suppresor protein MERLIN located on chromosome 22q12 Macroscopically the tumour appears as a firm yellowish encapsulated mass with the nerve splayed out on its surface. Histologically the tumour consists of packed sheaves of connective tissue cells with intercellular vacuoles and cysts (reticular pattern). Haemorrhage can occur (particularly in the reticular type), leading to a sudden increase in size.
- 7. Classification Of Vestibular Schwanoma
- 8. TUMOR DEVELOPMENT Develops in nerve sheath Compresses rather than invading the nerve Gradually fills all the IAC & Extrameatal expansion Tumour extend into cerebellopontine angle Tumour compress on CN V tumour compressing on CN V, IX, X, XI Pressure over brainstem and cerebellum
- 9. Clinical features Clinically, two phases can be recognized Otological phase in which a small tumour compresses structures in the meatus Neurological phase as the tumour expands medially into the cerebellopontine angle.
- 10. Otological symptoms Gradual and progressive unilateral deafness is the usual presenting symptom (90%). The deafness is often associated with tinnitus (70%). Sudden onset hearing loss can occur (10%). Some patients have normal hearing (5%). Vertigo is an unusual complaint
- 11. Neurological symptom 5th CN: Earliest sign is impaired corneal reflex. Motor functions are affected rarely. Facial pain, numbness and paraesthesiae may occur. 7th CN: Sensory first; loss of sensation in the postero-superior aspect of EAC called (Hitselberger sign). 9th and 1oth CN: hoarseness with dysphagia .palatal, pharyngeal and laryngeal paralysis. Late symptom: Ataxia and unsteadiness develop with progressive brain stem displacement and cerebellar involvement.
- 12. INVESTIGATIONS
- 13. Radiological investigations. magnetic resonance imaging (MRI) with gadolinium enhancement is the gold standard for diagnosis of VC Medium-sized tumors (3 cm) resemble an ice cream cone on MRI These tumors enhance intensely with contrast CT-scan; can not detect intermeatal tumors. but should only be used when MRI is unavailable
- 14. Other investigation Pure tone audiometry - PTA shows assymmetric , down sloping , high frequency SNHL in almost 70% of patients Speech discrimination score (SDS) Acoustic reflex decay ABR test- ABR is partially or completely absent , or there is a delay in latency of wave V on the affected side Evoked response audiometry (BERA)- It is very useful in the diagnosis of retrocochlear lesions. CSF examination
- 15. Treatment option Patient’s age and medical condition Size and the location of the tumor Auditory and vestibular function of the tumor side and the contralateral side. Tumor progression Surgeon’s preference
- 16. Treatment option Observation With Serial Imaging Stereotactic Radiation Microsurgeries
- 17. OBSERVATION Age >65years, preferred Patients with vestibular shwannoma in the only hearing ear with serviceable hearing and no imminent risk to brainstem function. Tumour growth is monitored . Serial imaging at 6 months interval is done , if no growth is seen then yearly
- 18. STEREOTACTIC RADIATION A high dose of radiation can be delivered to a defined region, usually within a well- immobilized system that conforms closely to the target volume. Various modalities are: Gamma knife LINEAC: Linear Accelerator Photon Radiation Therapy Proton Beam Therapy
- 19. Surgery Translabryinthine Middle cranial fossa approach Sub occipital (retro sigmoid) approach Combined
- 21. THANK YOU