2. Schwann cells
• Schwann cells are the glial cells of PNS(oligodendrocytes
in CNS) Can be myelinated or non myelinated.
• They support the neuron .
3. RELATED ANATOMY
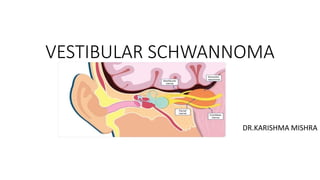
• INTERNAL ACOUSTIC MEATUS
Internal auditory canal (IAC) is
about 1 cm long and passes
into petrous part of temporal
bone in a lateral direction.
It is lined by dura.
At its lateral end (fundus) IAC is
closed by a vertical
cribriform plate of bone that
separates it from labyrinth.
4. • A transverse crest divides this plate into smaller upper and larger
lowerparts.
• Upper part is further divided into anterior and posterior quadrant by
a vertical crest called Bill’s bar.
5.
6. CP ANGLE
• Triangular shaped
• Filled with CSF
• Sup – tentorium
• Inf – cerebellar tonsil & medullary olives
• Ant – posterior dural surface of petrous bone
& clivus
• Post – ventral surface of pons & cerebellum
• Med – cisterns of pons & medulla
• Apex – lateral recess of 4 th ventricle
• Foramen of luschka – lateral opening of 4 th
ventricle opens into CPA
7. INTRODUCTION
• Unilateral vestibular schwannoma (VS) is a
benign tumour arising from abnormally
proliferative schwann cells, which envelope
the lateral portion of the vestibular nerve in
the internal acoustic meatus.
• Bilateral vs is seen in Nf2
• At a consensus conference it was
determined that the term ‘acoustic
neuroma’, often used in the past to describe
this entity, should be replaced by the more
accurate term ‘vestibular schwannoma’
8. PATHOGENESIS
• VS originate from the nerve sheath-the schwann
cells of the SUPERIOR VESTIBULAR(SVN) OR
INFERIOR VESTIBULAR NERVE(IVN) at the
transition zone of the peripheral and central
myelin.(Obsteiner-Redlich zone)- boundry
between pns and cns /boundry between schwann
cell and oligodentrocytes
• The transition zone is present in the lateral part
of CPA or medial part of IAC.
• VSs most commonly arise in the IAC than CPA.
• The reason that VSs mostly arise from vestibular
nerves is due to highest concentration of schwann
cells in the vestibular ganglia in the IAC.
9. • VSs occur due to mutations in gene for the tumor suppressor protein
merlin,located on chromosome 22q12.
• In NF2, patients inherit 1 mutated allele and 1 normal allele (in
contrast to sporadic cases where both are inherited normal and
requires mutation in both copies to get VS)
10. • The tumour develops in the nerve sheath, it
compresses rather than invades the nerve on
which it arose, thereby leaving a plane between
the nerve fibres and the tumour.
• As the VS grows, it gradually fills all the internal
acoustic meatus and eventually protrudes out of
the porus
• Bone resorption is an active, slowly progressive
process, caused presumably by increased
vascularization, fibrosis and adhesions in the
tumour area, where the pressure from the
tumour, due to its growth, plays an important role
11. NATURAL HISTORY
• Slow rate of growth in IAC and then into the cistern of the CPA. (VERY
SLOW PROGRESSIVE TUMOR)
• Periods of growth intermixed with periods of quiescence.
• Average growth rate is 1.8 mm/yr.
• This slow growth is the reason for insidious and progressive symptoms
and signs as there is displacement, distortion and compression of
structures first in the IAC and then in the CPA.
• Occasionally rapid expansion may occur due to cystic degeneration or
haemorrhage into the tumor, causing rapid neurologic deterioration.
• Initial growth affects vestibulocochlear nerve in IAC and causes U/L
hearing loss, tinnitus & vertigo. (typical features of any lesion in CPA)
12. Schematic illustration of initial
growth and intrameatal
expansion of VS. A, acoustic
nerve in the fundus; B,
brainstem; C, cerebellum; V,
superior and inferior nerves in
the fundus; VE, fourth ventricle;
5, trigeminal nerve; 7, facial
nerve; 8, acousticovestibular
nerve.
13. • Extra-meatal expansion of the tumour into the relatively large and
empty pontine cistern initially develops silently. Growth and extension
in this direction causes some displacement and stretching of the VIIth
and VIIIth cranial nerves on the anterior aspect of the tumour and of
the anterior inferior cerebellar artery (AICA) on the inferior aspect.
14.
15. • After further growth, the tumour expands sufficiently to touch and
compress the cerebellum and trigeminal nerve. During this process, the
VIIth and VIIIth nerves are thinned or ribboned, become compressed and
even more stretched.
• At the same time, the internal acoustic meatus continues to become more
and more widened. Further growth and expansion causes compression
and displacement of the brainstem and the fourth ventricle, which leads
gradually to hydrocephalus
16. CLASSIFICATION OF VS (SIZE)
At the Consensus Meeting on Reporting Systems on Vestibular Schwannoma in 2003,
the classification scheme according to size
17. SYMPTOMS
• HEARING LOSS
• In more than 90% of patients, the first symptom is unilateral
progressive hearing loss with or without tinnitus. (In 5–10% of cases,
hearing loss is sudden and may be profound).
• Classically, there is
• a slowly progressing
• retrocochlear hearing loss, which is more pronounced in the higher
end of the auditory range and is often accompanied by
• poor speech discrimination
18. • Vestibular
• Self limiting episodes of vertigo in 60% - patients tolerate and adapt well to
the disequilibrium because of the central compensation for slowly
• Trigeminal
• Midfacial numbness (V2)
• Absent corneal reflex evolving vestibular injury
• Facial
• 17% of patients
• Sensory 1st affected – numbness in posterior wall of external canal wall
called hitzelberger sign.
19. • CN II, IV & VI
• Decreased visual acuity, Diplopia
• Hydrocephalus
• Headache, nausea, vomiting, altered mental status
• CN IX & X
• Dysphagia, aspiration, hoarseness,
• Poor gag reflex, VC paralysis
20. PATHOLOGY
• Smooth surface, yellow to gray
colour.
• Usually solid.
• Occasional cystic components.
• Firm to soft in consistency
depending on components.
21. 2 regions are noted intermixed – Antoni A
& Antoni B.
• Antoni A – densely packed cells with
spindle shaped nuclei and fibrillary
cytoplasm. The palisades of the nuclei are
termed Verocay bodies.
• Antoni B - hypocellular areas containing
vacuolated, pleomorphic cells.
• VS sections stain with S-100
immunoperoxidase
22. CYSTIC VESTIBULAR SCHWANNOMA
• Cyst formation within VS is seen regularly and is easily detected by MR.
This has been thought to represent degenerative change or coalescence of
microcysts in Antoni A tissue. More recently, it has been shown that cystic
tumours contain an increased amount of Antoni B tissue that is surrounded
by a membrane-like structure composed of Antoni A type cells.
• Therefore, three criteria are required to be present before a tumour can be
termed ‘cystic’.
1)There must be a hypodense/hypointense area on CT/MR.
2) Perioperative identification of the cystic elements must be achieved
3) There must be histological verification of S-100 positive membrane
23. • The surgical outcome of cystic VS is less favourable than that of solid
tumours of comparable size.
• The cystic elements expand, causing displacement of the brainstem
and compression of the fourth ventricle and hydrocephalus.
25. HISTORY TAKING
• Progressive unilateral sensorineural hearing loss, often accompanied
by tinnitus, is the presenting symptom in majority of cases. There is
marked difficulty in understanding speech, out of proportion to the
pure tone hearing loss. This feature is characteristic of acoustic
neuroma.
• Nf history in family should be asked
• Age -40 to 60yrs
• True vertigo rarely seen
• Very slow progressive,patient have tumor for several years without
marked symptoms.
26. AUDIOMETRIC TESTS
• PTA – asymmetric, down-sloping, high-
frequency, SNHL in 70%.
• SDSs are lower than predicted by pure-
tone thresholds, which are further
accentuated when retested at higher
speech intensity. This phenomenon is
called roll over. Seen in nearly 50%
• Delayed latency of wave 5 or absent wave
5 in Bera
27. IMAGING
• MRI with Gadolinium (Gd)contrast
– gold standard
• A series of T1W images, T1W with
Gd, T2W images are obtained. (T1W
– CSF dark & fat bright, T2W – CSF
bright).
• A hypointense globular mass in
T1W with Gd images is
characteristic.
• High resolution fast spin echo T2W
scans are being developed in which
CSF is used as a contrast.
31. Patient selection
TRANSLABYRINTHINE APPROACH
• Tumor > 2.5cm in maximal dimension
• All cases of nonservicable hearing
• MIDDLE CRANIAL FOSSA APPROACH
• Tumor confined to IAC
• Servicable hearing
• RETROSIGMOID APPPROACH
• Tumor primarily in CPA,minimal extension to IAC
• Good hearing
Servicable hearing:
PTA average threshold better than 50 db,a sds better than 50 db or both
This is known as 50/50 rule
32. TRANSLABYRINTHINE APPROACH
• ADVANTAGES
• No cerebellar retraction
• Early facial nerve identification
• Exposure of entire facial nerve
• DISADVANTAGES
• Destroys residual hearing completely
• CSF fistula
33. Steps of translabyrinthine approach:
1. Skin and periosteal flaps
2. Extended cortical mastoidectomy
3. Bony labyrinthectomy
4. Skeletonization of the jugular bulb and vertical portion of the facial nerve
5. Skeletonization of the IAM
6. Identification of the facial nerve at the lateral end of the internal meatus
7. Opening of the posterior fossa through the dura of the posterior surface of
the petrous bone
8. Removal of tumour using standard neurosurgical techniques
9. Closure with obliteration of the middle ear and petrosectomy defect,
usually with abdominal fat.
34. • Boundaries of the approach –
1. Ant – facial nerve & cochlear duct
2. Sup – middle fossa dura
3. Post – posterior fossa dura
4. Inf – jugular foramen
35. • A curved incision above and behind thepinna is planned, it can be
about 3-4 cm behind the postauricular sulcus.
36. • Extended cortical mastoidectomy done.
• The wide bone removal over the middle fossa dura and the sigmoid
sinus, allowing the dura and the sinus to be retracted and the access
improved
37. A complete labyrinthectomy is then
performed
with medial skeletonization of
middle & posterior
fossa dura and decompression of the
sigmoid sinus to the jugular foramen
38. The internal meatus has been skeletonized
and the intrameatal portion of the tumour
exposed
39. • After bony skeletonisation of IAC, dura of
IAC is opened and facial nerve is identified
medial to the vertical crest (bills bar) in the
fundus or lateral aspect of IAC.
• Tumor removal is done from lateral to
medial along the IAC.
• In large tumors, it is debulked internally
and then capsule is removed from
surrounding structures including facial
nerve.
• Abdominal fat is placed at the defect site
The tumour is
dissected off the facial nerve (FN) in a lateral
to medial direction.
40. MIDDLE FOSSA APRROACH
• Advantages
1) fully exposes lateral third of internal auditory canal without sacrificing hearing
2) extradural.
It is the only procedure that fully exposes the lateral third of the internal auditory canal without sacrificing
hearing.
• Disadvantages
1) CN7 is in way during tumor removal (CN7 courses across anterior superior portion of tumor) - temporary
postoperative paresis is more common.
2) temporal lobe must be retracted → temporal lobe injury (especially troublesome with dominant side).
3) risk of dural laceration in elderly patients.
4) very limited exposure of posterior fossa; also may leave tumor laterally.
5) technically difficult.
6) postoperative trismus (related to manipulation and/or injury to temporalis muscle).
41. • 1. Skin and soft tissue incisions
• 2. Middle fossa craniectomy
• 3. Extradural approach to upper surface of temporal
• bone and to posterior fossa
• 4. Skeletonization of internal meatus
• 5. Identification of facial and vestibular nerves
• 6. Removal of tumour
• 7. Closure
42. RETROSIGMOID APPROACH
Advantages
1.Hearing preservation
2. Versatile approach to CPA & IAC
3.No limit to size of tumor
Disadvantages –
1. Persistent post-op headache
2. Increased difficulty in resolving CSF leaks
3. Need for cerebellar retraction
4. Inability to have direct access to facial nerve
5.Air embolism
43. • Modification of traditional suboccipital approach used by
neurosurgeons to address most posterior fossa lesions.
• It’s a versatile approach with a panoramic view of CPA from foramen
magnum inferiorly to tentorium superiorly.
• Medial 2/3 rd of IAC is also accessible without violating inner ear;
therefore, hearing is preserved.
44. Intra operative Complications
• Vascular injury
• Air embolism
• Parenchymal brain injury
• Cranial nerve injury
• Only venous drainage of temporal lobe – vein of labbe & lower
portion of cerebellum are vulnerable.
• Retraction injury to cerebellum during retrosigmoid & to temporal
lobe during middle fossa approach can occur
45. Post op complications
• Hemorrhage, Stroke, VTE, SIADH, CSF leak, Meningitis.
• Post op haemorrhage manifest as neurologic & cardiovascular
deterioration and will require evacuation.
• Post-op LMW heparin with compression stockings & intermittent
pneumatic compression devices will reduce risk of TE without increasing risk
of intracranial bleed.
• Most common complication is CSF leak (10-15%) , may occur via the
wound or via a pneumatic pathway to ET. These leaks resolve with
conservative care – placing sutures at leak site, replacing the mastoid
dressing, decreasing ICP with acetazolamide, restricting fluid intake and
resting in bed.
• Meningitis (2-10%) – aseptic / bacterial / lipoid due to irritation from fat
graft
46. • SUMMARY –
• All 3 approaches have mortalirty < 1% , >90% rate of tumor removal
& facial nerve preservation.
• Translabyrinthine – 98% facial nerve preservation
• Hearing preservation – 50% in retrosigmoid & 70% in middle fossa
approach.
• Recurrence rate < 1.5%
47. Streotactic Radiation
• Goal – prevent further growth of VS while preserving hearing & facial
nerve function.
• Mechanism relies on delivering radiation to a specific intracranial
target by using several precisely collimated beams of ionising radiation.
• Beams take various pathways to the target tissue, creating a sharp
dose gradient between the target tissue & surrounding tissue.
• Ionising radiation causes necrosis & vascular fibrosis.
• Time course of effect is over 1-2 years.
• Ionising radiation is most commonly delivered by 201-source cobalt
60 gamma knife system
48. • Radiation therapy is useful in patients in whom arrest of tumor
growth is acceptable.
• These patients have either short life expectancies or high surgical risk.
• Stereotactic radiotherapy may improve hearing preservation in
patients with 2-3 cm VSs compared to microsurgery.
• Radiation therapy in large (>3cm) tumors or those causing brain
compression will exacerbate symptoms owing to initial tumor swelling
initial tumour arising from the vestibular nerve. (b) Tumour expanded to fill most of the internal acoustic meatus.c) Meatus, with some bone resorption,
widened and filled out with the tumour, slightly protruding out
of the porus.
Schematic illustration of expansion of VS in the cerebellopontine angle. Abbreviations as in Figure 101.2. (a) Tumour
occupying half of the pontine cistern. (b) Tumour extending to the
cerebellum with some compression of the cerebellum. (c)
Tumour compressing the cerebellum, brainstem and trigeminal nerve.
Roll Over Phenomenon. It is seen in retrocochlear
hearing loss. With increase in speech intensity above a
particular level, the PB word score falls rather than main
tain a plateau as in cochlear type of sensorineural hearing
loss
Speech Discrimination Score. It is a measure of pa
tient’s ability to understand speech. Here, a list of pho
netically balanced (PB) words (single syllable words, e.g.
pin, sin, day, bus, etc.) is delivered to the patient’s each
ear separately at 30–40 dB above his SRT and the percent
age of words correctly heard by the patient is recorded. In
normal persons and those with conductive hearing loss
a high score of 90–100% can be obtained) Speech Reception Threshold (SRT). It is the mini
mum intensity at which 50% of the words are repeated
correctly by the patient.
2. Short Increment Sensitivity Index
(SISI Test)
Patients with cochlear lesions distinguish smaller chang
es in intensity of pure tone better than normal persons
and those with conductive or retrocochlear pathology.
SISI test is thus used to differentiate a cochlear from a
retrocochlear lesion.
In this test, a continuous tone is presented 20 dB above
the threshold and sustained for about 2 min
Speech Discrimination Score. It is a measure of pa
tient’s ability to understand speech. Here, a list of pho
netically balanced (PB) words (single syllable words, e.g.
pin, sin, day, bus, etc.) is delivered to the patient’s each
ear separately at 30–40 dB above his SRT and the percent
age of words correctly heard by the patient is recorded. In
normal persons and those with conductive hearing loss
a high score of 90–100% can be obtained)