Enhancing nutritional environments through access to fruit & vegetables in sc...
Nasrallah_FNCE2015
1. TeleTeam Care: Promoting Lifestyle and Behavioral Health for Uncontrolled Diabetic
Patients in Underserved Rural Communities via Telehealth
Background
Problems Addressed:
• Rural primary care providers are challenged with little or no
access to services that can assist in delivering much
needed chronic disease care to patients with diabetes and
behavioral challenges.
• Diabetes management and prevention of complications in
rural primary care is frequently exacerbated by profound
lifestyle and behavioral challenges that limit health
outcomes.
• Diabetics with behavioral problems have more diabetes
complications.
Demographics:
• High prevalence of diabetes in eastern NC
(11.3% vs. 9.8% in NC)
• Higher prevalence in African Americans
(16.7% vs. 10.2% in whites).
• Nearly 50% of patients with diabetes have co-morbid
behavioral challenges and require help with lifestyle
changes, medications, and/or counseling for concurrent
depression, anxiety, or adjustment disorders.
Purpose
Evaluate the clinical and pragmatic effectiveness of delivering
team-based care for underserved patients with diabetes and
behavioral challenges via telehealth into rural primary care
practices.
Attend to patients who have diabetes and co-morbid
behavioral challenges who are either insured through federally
subsidized funding, uninsured, or privately insured, but unable
to afford the high cost of specialist services and prescriptions.
Provide team-based care to patients with little knowledge of
diabetes self-management practices and limited exposure to
diabetes education.
Methodology
TeleTeam Team-Based Delivery Care
Coordination of Patient Referrals and Subsequent Encounters
• Utilize basic screening instrument at rural primary care practice site to
identify patients who have one or more self-management challenges.
• Diet and lifestyle, blood glucose control, medication, and depression
and/or anxiety.
• Communicate with project coordinator to initiate “point-of-care” telehealth
consultation or schedule future appointments.
• Arrange follow-up visits by collaborative discussion among the patient,
rural primary care staff, and specialist provider(s) and evaluate progress
of patients.
• Healthy eating, being active, monitoring, taking medications, problem
solving, reducing risk, and health coping.
Referrals to TeleTEAM Specialty Services
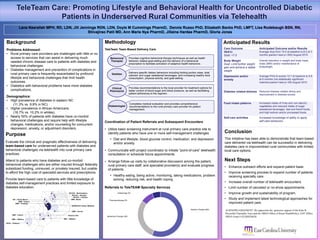
Anticipated Results
Conclusion
This initiative has been able to demonstrate that team-based
care delivered via telehealth can be successful in delivering
diabetes care in impoverished rural communities with limited
local care options.
Next Steps
• Enhance outreach efforts and expand patient base.
• Improve screening process to expand number of patients
receiving specialty care.
• Increase overall number of telehealth encounters.
• Limit number of canceled or no-show appointments.
• Improve growth and sustainability of program.
• Study and implement latest technological approaches for
improved patient care.
Care Outcome Anticipated Outcome and/or Results
HbA1c
Goal: <7.0
Average drop from 10.0 at baseline to 8.5 at 3
months (paired t-test p<.000) August 2015
Body Weight
Goal: Limit further weight
gain and achieve a stable
weight
Overall reduction in weight and body mass
index (BMI) and/or maintenance of
bodyweight.
Depression and/or
anxiety
Average PHQ-8 scored 10.7 at baseline to 6.8
at 6 months (not statistically significant
matched paired t-test p<.09) August 2015
Diabetes related-distress Reduced disease related stress and
improvement in distress scores.
Food intake patterns Increased intake of fruits and non-starchy
vegetables and reduced intake of sugar
sweetened beverages, fast and friend foods,
and high sodium and/or processed foods.
Self-care activities Increased knowledge of ability to apply
self-care behaviors.
Provides cognitive behavioral therapy techniques as well as health
behavior related goal-setting and the delivery of a behavioral
prescription to facilitate activation of adaptive health behaviors.
Delivers specific dietary behaviors including limiting portion sizes, total
calories, and sugar sweetened beverages, and increasing healthy food
consumption, physical activity, and goal-setting.
Provides recommendations to the local provider for treatment options for
better control of blood sugar and blood pressure, as well as facilitating
patient adherence to the regimen.
Behavioral
Therapist
Clinical
Pharmacist
Dietitian
Lana Nasrallah MPH, RD, LDN, Jill Jennings RDN, LDN, Doyle M Cummings PharmD, Dennis Russo PhD, Elizabeth Banks PhD, LMFT, Lisa Rodebaugh BSN, RN,
Shivajirao Patil MD, Ann Marie Nye PharmD, Jillaine Hardee PharmD, Gloria Jones
ACKNOWLEDGEMENT: We appreciate the generous support of the Kate B.
Reynolds Charitable Trust and the HRSA Office of Rural HealthPolicy; OAT Office;
HRSA Grant # H2ARH26028
VMG– Bertie
BSOM ECU Family Medicine
VMG – Aurora
VMG– Tarboro
VMG – Pinetops
GMC – Wallace VMC – Wallace
GMC – Faison Kinston CHC
RCCHC - Murfreesboro
RCCHC – Ahoskie
RCCHC – Colerain
OIC – Rocky Mount
RHCC - Robeson
Completes medical evaluation and provides comprehensive
recommendations to the rural primary care provider for patient
management.
Diabetologist
Nutrition Therapy 56%
Diabetology 6%
Pharmacotherapy 9%
Behavioral Therapy 29%