Aortic regurgitation pathophysiology
•Download as PPTX, PDF•
2 likes•818 views

Brief Introduction

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Aortic regurgitation pathophysiology
Similar to Aortic regurgitation pathophysiology (20)
More from Kunwar Saurabh
More from Kunwar Saurabh (20)
Recently uploaded
Recently uploaded (20)
Aortic regurgitation pathophysiology
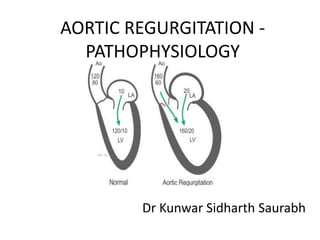
- 1. AORTIC REGURGITATION - PATHOPHYSIOLOGY Dr Kunwar Sidharth Saurabh
- 3. ETIOLOGY
- 6. PATHOPHYSIOLOGY • VOLUME LOAD – COMPENSATORY MECHANISMS – LV END DIASTOLIC VOLUME INCREASES TO ACCOMMODATE REGURGITANT VOLUME – ALONG WITH INCREASE IN CHAMBER COMPLIANCE – HENCE, THERE IS NO INCREASE IN DIASTOLIC FILLING PRESSURE
- 7. Cont.. – INCREASE IN EDV INCREASE TOTAL STROKE VOLUME – HENCE, FORWARD STROKE VOLUME MAINTAINED WITHIN NORMAL RANGE – ALSO, ADAPTATION TO VOLUME OVERLOAD IS BY NEW SARCOMERES CAUSING “ECCENTRIC LV HYPERTROPHY”
- 8. Cont.. LV PRELOAD INCREASES PRELOAD AT SACRCOMERE LEVEL IS NEAR NORMAL CONTRACTILE FUNCTION PRESERVED ENHANCED TOTAL STROKE VOLUME
- 9. Cont.. AUGMENTED CHAMBER VOLUME INC SYSTOLIC WALL STRESS AND AFTERLOAD AFTERLOAD INCREASE IN STIMULUS FOR CONCENTRIC HYPERTROPHY
- 10. Cont.. • THUS “AR – CHRONIC” IS A CONDITION OF COMBINED – VOLUME OVERLOAD – PRESSURE OVERLOAD • HENCE THERE IS BOTH – – ECCENTRIC HYPERTROPHY – CONCENTRIC HYPERTROPHY
- 11. POINTS TO NOTE - • DUE TO COMPENSATORY PROCESSES- – PATIENT MAY REMAIN ASYMPTOMATIC FOR DECADES – AFTER LOAD REDUCTION THERAPY HAS POTENTIAL TO REDUCE DEGREE OF REGURGITATION VIA – • REDUCES AFTERLOAD AND COMPENSATORY DILATATION AND HYPERTROPHY
- 12. Cont.. • In some patients compensatory process cannot be maintained for long • Results in LV systolic dysfunction • Symptoms of dyspnoea and fatigue often develops at this transition point. • Process is mostly insiduos
- 13. IMPORTANT TO NOTE LV SYSTOLIC DYSFUNCTION AFTERLOAD MISMATCH REVERSIBLE AVR CAUSES COMPLETE REVERSAL IMPAIRED MYOCARDIAL CONTRACTILITY IRREVERSIBLE
- 14. NATURAL HISTORY • It can be divided into - – Patients with normal LV systolic function – Patients with LV systolic dysfunction
- 15. With normal LV Systolic function • These patients remain asymptomatic for decades. • Charecterised by very gradual rate of deterioration to symtoms. • Likelihood of developing symptoms – 4.3%/yr • Average mortality rate – 0.2%/yr
- 16. Cont .. • Most important aspect of evaluation – detailed history. • However, 25% pt may decompensate without significant history. • Implies the importance of noninvasive evaluation. • Factors associated with high risk – – Age – Lved - >50mm – 19% , 40-50mm – 6%, <40mm -nil – LVes
- 17. With LV systolic dysfunction • Much more aggressive natural history. • Become candidate for operation because of symptoms, within a few years. • If asymp symptomatic , require operation within 2-3 years.
- 18. Clinical presentation • Absence of complications, asymptomatic for decades • May have some episodes of orthostatic dizziness • May be aware of increased vigor of contraction of lv while lying down or audible heart tones. • May have anginal pain – – Low aortic diastolic pressure and inc myocardial demands – Atherosclerosis – Luetic
- 19. Cont .. • CHF – Most common symptom • LV failure precedes RV failure. • Decreased exercise tolerance, dyspnoea. • Orthopnea , PND • Dyspnoea may be releived with eventual RV failure without TR. • Palpitations – usually not due to arrythmia
- 20. Cont .. • Complications which may worsen porgnosis – – Infectious endocarditis – Ostial narrowing – Co-existing CAD – Atrial or ventricular arrythmias
- 21. Physical Findings • DBP low. • Kortokoff sounds may be heard even when the cuff pressure reaches zero • Wide pulse pressure. • Sinus tachycardia. • Apical impulse is displaced to left and below its usual location • Murmur – soft, blowing, holodiastolic, decresendo
- 22. Cont .. • Duration of murmur related to severity. • Systolic ejection murmur may be present. • Carotid thrill is present in considerable number of patients. • Austin Flint Murmur – late diastolic rumbling murmur
- 23. Peripheral signs. • Corrigans Pulse - water hammer pulse • Mayne’s sign – fall in DBP >20mmhg on raising arm
- 24. De musset sign, Muller’s Sign
- 25. Lighthouse Sign – Blanching of forehead
- 26. Ashrafian Sign- pulsatile pseudo- proptosis
- 27. Landolfi Sign – Pupillary Contraction
- 28. Beckers sign
- 29. Quinckie’s sign
- 30. Signs in Lower extremities
- 31. Rosenbach Sign
- 32. Gerhardts sign – pulsating spleen
- 33. Shileys Sign – Pulsating Cervix
- 34. INVESTIGATIONS • ECG – – LEFT VENTRICULAR PREPONDERANCE – SMALL Q, TALL R, ISOELECTRIC ST SEG. AND UPRIGHT T – DIASTOLIC OVERLOAD – ST DEPRESSION, T INVERSION – SYSTOLIC OVERLOAD – AR SEC. TO INFLAMTORY PROCESS – BLOCKS, LONG PR ETC
- 35. CXR • CARDIOMEGALY • “BOOT SHAPED” • PROMINENT ASCENDING AORTA • EGG SHELL LINEAR CALCIFICATION ALONG ASCENDING AORTA – LUETIC • CALCIFICATION – RHD, BICUSPID, UNICUSPID • LVF – PULMONARY VASCULAR REDISCTRIBUTION
- 36. CXR
- 37. ECHO • IN ABSENCE OF MITRAL DISEASE – BROAD BAND OF (3-4MM) DIASTOLIC FLUTTER (20- 70HZ) OR VIBRATION OF ANTERIOR MITRAL LEAFLET. • MITRAL VALVE CLOSURE PRIOR TO QRS. • DIALATED AORTIC ROOT • LVED, LVES DIMENSIONS, EF • DOPPLER TECHNIQUE
- 41. CARDIAC CATH • HAEMODYNAMIC MEASUREMENTS • WITH SEVERE DECOMPENSATION – LT VENTRICULAR END DIASTOLIC AND AORTIC DIASTOLIC PRESSURES EQUALISE • LEFT VENTRICULOGRAPHY – – INC EDV – ECCENTRIC LVH – REDUCED CONTRACTILE FUNCTION – ABNORMAL END SYSTOLIC VOLUME AND END SYSTOLIC PRESSURE RELATIONSHIP
- 42. CONT.. • MORE ACCURATE METHOD – CALCULATE REGURGITANT FRACTION • REGURG FRACTION = TOTAL CO FROM LEFT VENTRICULOGRAM – FORWARD CO BY FICK TECHNIQUE – MILD TO MOD- <0.50 • SEVERE - >0.50
- 43. THERAPY • MOST IMPORTANT DETERMINANT – – PREOP LV SYSTOLIC FUNCTION – OTHERS – – FRACTIONAL SHORTENING – END SYSTOLIC DIMENSIONS
- 44. ROLE OF VASODILATOR THERAPY • REDUCE REGURGITANT VOLUME HENCE – – REDUCE LVed, WALL STRESS, AFTERLOAD • MAINLY DRUGS USED ARE – – SNP – HYDRALAZINE – NIFEDIPINE • RATIONALE – BENEFICIAL HAEMODYNAMICS SHOULD TRANSLATE TO PROLONGATED COMPENSATED PHASE • MAY RESULT ONLY AS “COSMETIC EFFECT” • EVEN SLIGHTLY DEPRESSED LV FUNCTION NECESSITATE AVR • REMEMBER, ITS NOT AN ALTERNATIVE TO AVR
- 45. INDICATION FOR AVR • AVR, ONLY IF THE DEGREE IS SEVERE • LV DYSFUNCTION – AVR • CO EXISTING CONDITION – AVR • ONSET OF TRUE CARDIAC SYMPTOMS EVEN MILD – AVR • A DEC IN EF DURING EXERCISE IS A VERY NON SPECIFIC FINDING.