Lung Cancer: Precise Prediction

OBJECTIVE: 5-survival (5YS) and life span after radical surgery for non-small cell lung cancer (LC) pa¬tients (LCP) (T1-4N0-2M0) was analyzed. METHODS: We analyzed data of 771 consecutive LCP (age=57.6±8.3 years; tumor size=4.1±2.4 cm) radically operated and monitored in 1985-2022 (m=662, f=109; upper lobectomies=278, lower lobectomies=178, middle lobectomies=18, bilobectomies=42, pneumonectomies=255, mediastinal lymph node dissection=771; combined procedures with resection of trachea, carina, atrium, aorta, VCS, vena azygos, pericardium, liver, diaphragm, ribs, esophagus=194; only surgery-S=620, adjuvant chemoimmunoradiotherapy-AT=151: CAV/gemzar + cisplatin + thymalin/taktivin + radiotherapy 45-50Gy; T1=322, T2=255, T3=133, T4=61; N0=518, N1=131, N2=122, M0=771; G1=195, G2=243, G3=333; squamous=418, adenocarcinoma=303, large cell=50; early LC=215, invasive LC=556; right LC=413, left LC=358; central=291; peripheral=480. Variables selected for study were input levels of 45 blood parameters, sex, age, TNMG, cell type, tumor size. Regression modeling, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine significant dependence. RESULTS: Overall life span (LS) was 2240.9±1748.8 days and cumulative 5-year survival (5YS) reached 73%, 10 years – 64.2%, 20 years – 43%. 503 LCP lived more than 5 years (LS=3126.6±1536 days), 145 LCP – more than 10 years (LS=5068.5±1513.2 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (77.7% vs.63.4%, P=0.00001 by log-rank test). AT significantly improved 5YS (64.4% vs. 34.8%) (P=0.00003 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.035). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), eosinophils/CC (4), erythrocytes/CC (5),healthy cells/CC (6), segmented neutrophils/CC (7), lymphocytes/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0). CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data.
Recommended

Recommended
More Related Content
Similar to Lung Cancer: Precise Prediction
Similar to Lung Cancer: Precise Prediction (20)
More from Oleg Kshivets
More from Oleg Kshivets (15)
Recently uploaded
Recently uploaded (20)
Lung Cancer: Precise Prediction
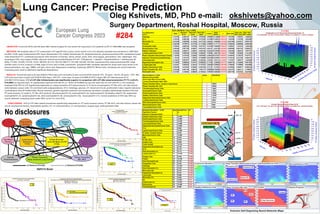
- 1. Lung Cancer: Precise Prediction No disclosures OBJECTIVE: 5-survival (5YS) and life span after radical surgery for non-small cell lung cancer (LC) patients (LCP) (T1-4N0-2M0) was analyzed. METHODS: We analyzed data of 771 consecutive LCP (age=57.6±8.3 years; tumor size=4.1±2.4 cm) radically operated and monitored in 1985-2022 (m=662, f=109; upper lobectomies=278, lower lobectomies=178, middle lobectomies=18, bilobectomies=42, pneumonectomies=255, mediastinal lymph node dissection=771; combined procedures with resection of trachea, carina, atrium, aorta, VCS, vena azygos, pericardium, liver, diaphragm, ribs, esophagus=194; only surgery-S=620, adjuvant chemoimmunoradiotherapy-AT=151: CAV/gemzar + cisplatin + thymalin/taktivin + radiotherapy 45- 50Gy; T1=322, T2=255, T3=133, T4=61; N0=518, N1=131, N2=122, M0=771; G1=195, G2=243, G3=333; squamous=418, adenocarcinoma=303, large cell=50; early LC=215, invasive LC=556; right LC=413, left LC=358; central=291; peripheral=480. Variables selected for study were input levels of 45 blood parameters, sex, age, TNMG, cell type, tumor size. Regression modeling, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine significant dependence. RESULTS: Overall life span (LS) was 2240.9±1748.8 days and cumulative 5-year survival (5YS) reached 73%, 10 years – 64.2%, 20 years – 43%. 503 LCP lived more than 5 years (LS=3126.6±1536 days), 145 LCP – more than 10 years (LS=5068.5±1513.2 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (77.7% vs.63.4%, P=0.00001 by log-rank test). AT significantly improved 5YS (64.4% vs. 34.8%) (P=0.00003 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.035). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), eosinophils/CC (4), erythrocytes/CC (5),healthy cells/CC (6), segmented neutrophils/CC (7), lymphocytes/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0). CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: PT early-invasive cancer; PT N0--N12; cell ratio factors; blood cell circuit; biochemical factors; hemostasis system; AT; LC characteristics; LC cell dynamics; surgery type; anthropometric data. Oleg Kshivets, MD, PhD e-mail: okshivets@yahoo.com Surgery Department, Roshal Hospital, Moscow, Russia a #284 Cox Regression n=771 Chi2= 350.946 df = 16 p = 0.0000 Beta Standard Error Beta 95% lower Beta 95% upper t-value Wald Statist. p Risk ratio Risk ratio 95% lower Risk ratio 95% upper Histology 0.33762 0.085107 0.17081 0.504426 3.96698 15.73689 0.000073 1.401606 1.186267 1.656035 G1-3 0.30328 0.086196 0.13434 0.472225 3.51856 12.38023 0.000435 1.354299 1.143786 1.603558 Monocytes (%) -0.07548 0.029458 -0.13322 -0.017742 -2.56224 6.56506 0.010405 0.927300 0.875277 0.982415 Glucose -0.26756 0.076674 -0.41784 -0.117282 -3.48957 12.17711 0.000484 0.765244 0.658468 0.889335 Prothrombin Index 0.02843 0.006704 0.01529 0.041573 4.24106 17.98658 0.000022 1.028841 1.015410 1.042449 Recalcification Time -0.00492 0.001709 -0.00827 -0.001574 -2.88121 8.30139 0.003964 0.995089 0.991763 0.998427 Heparin Tolerance 0.00340 0.000677 0.00207 0.004726 5.02251 25.22560 0.000001 1.003405 1.002075 1.004737 Lymphocytes/Cancer Cells 0.15234 0.068349 0.01838 0.286301 2.22885 4.96778 0.025831 1.164556 1.018548 1.331493 Phase Transition Early-Invasive Cancer -1.42494 0.316782 -2.04582 -0.804055 -4.49816 20.23347 0.000007 0.240524 0.129275 0.447511 Adjuvant Chemoimmunoradiotherapy -1.15154 0.197372 -1.53839 -0.764699 -5.83436 34.03981 0.000000 0.316149 0.214728 0.465474 Leucocytes (tot) 0.12012 0.051077 0.02002 0.220234 2.35183 5.53111 0.018687 1.127637 1.020217 1.246368 Segmented Neutrophils (tot) -0.12022 0.056934 -0.23181 -0.008634 -2.11162 4.45892 0.034727 0.886723 0.793096 0.991403 Lymphocytes (tot) -0.22461 0.063032 -0.34815 -0.101074 -3.56350 12.69853 0.000366 0.798825 0.705990 0.903866 Healthy Cells/Cancer Cells -0.02439 0.010525 -0.04502 -0.003763 -2.31747 5.37067 0.020484 0.975903 0.955977 0.996244 Phase Transition N0---N12 0.83346 0.087102 0.66275 1.004177 9.56884 91.56266 0.000000 2.301270 1.940111 2.729661 Eosinophils (tot) -0.41281 0.126263 -0.66029 -0.165344 -3.26948 10.68949 0.001079 0.661785 0.516704 0.847603 Neural Network: n=702 Baseline Error=0.000; Area under ROC Curve=1.000; Correct Classification Rate 100% Rank Sensitivity Phase Transition Early---Invasive Lung Cancer 1 35878 Phase Transition N0---N12 2 28620 Thrombocytes/Cancer Cells 3 18847 Eosinophils/Cancer Cells 4 15521 Erythrocytes/Cancer Cells 5 15292 Healthy Cells/Cancer Cells 6 13792 Segmented Neutrophils/Cancer Cells 7 10113 Lymphocytes/Cancer Cells 8 9038 Stick Neutrophils/Cancer Cells 9 8716 Monocytes/Cancer Cells 10 6691 Leucocytes/Cancer Cells 11 5484 Bootstrap Simulation n=702 Significant Factors (Number of Samples=3333) Rank Kendall’Tau- A P< Healthy Cells/Cancer Cells 1 -0.849 0.000 Erythrocytes/Cancer Cells 2 -0.800 0.000 Thrombocytes/Cancer Cells 3 -0.705 0.000 Leucocytes/Cancer Cells 4 -0.596 0.000 Segmented Neutrophils/Cancer Cells 5 -0.564 0.000 T1-4 6 0.562 0.000 Lymphocytes/Cancer Cells 7 -0.529 0.000 PT Early---Invasive Cancer 8 0.410 0.000 Monocytes/Cancer Cells 9 -0.296 0.000 ESS 10 0.242 0.000 PT N0---N12 11 0.219 0.000 Surgery Type 12 0.208 0.000 Tumor Growth 13 -0.134 0.000 Segmented Neutrophils abs 14 0.128 0.000 G1-3 15 0.118 0.000 Stick Neutrophils tot 16 0.112 0.000 Lymphocytes (%) 17 -0.108 0.000 Surgery Type 18 0.160 0.000 Protein 19 -0.159 0.000 Stick Neutrophils abs 20 0.105 0.000 Coagulation Time 20 0.104 0.000 Histology 21 -0.103 0.000 Stick Neutrophils (%) 22 0.102 0.000 Monocytes abs 23 0.102 0.000 Segmented Neutrophils tot 24 0.101 0.000 Leucocytes 25 0.098 0.001 Monocytes (%) 26 0.088 0.001 Hb 27 -0.081 0.01 Erythrocytes tot 28 -0.079 0.05 Erythrocytes 29 -0.066 0.05 Thrombocytes tot 30 0.060 0.05 Survival Function 5YS=73%; 10YS=64.2%; 20YS=43%. Complete Censored -5 0 5 10 15 20 25 30 Years after Surgery 0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 Cumulative Proportion Surviving Cumulative Proportion Surviving (Kaplan-Meier) Complete Censored 0 5 10 15 20 25 30 35 Years after Surgery -0.2 0.0 0.2 0.4 0.6 0.8 1.0 Cumulative Proportion Surviving Invasive LC Early LC Cumulative Proportion Surviving (Kaplan-Meier) Complete Censored 0 5 10 15 20 25 30 35 Years after Surgery 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 Cumulative Proportion Surviving N12 N0 Cumulative Proportion Surviving (Kaplan-Meier) Complete Censored 0 5 10 15 20 25 30 35 Years after Surgery -0.1 0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 Cumulative Proportion Surviving Pneumonectomies Lobectomies Cumulative Proportion Surviving (Kaplan-Meier) P=0.025 by Log Rank test Complete Censored 0 5 10 15 20 25 30 35 Years after Surgery 0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 Cumulative Proportion Surviving male female Cumulative Proportion Surviving (Kaplan-Meier) LCP with N12 5YS LCP after Adjuvant Treatment=63.4%; 5YS after surgery along=34.8%; P=0.00003 by Log-Rank Test. Complete Censored 0 5 10 15 20 25 30 Years after Surgery 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 Cumulative Proportion Surviving only Surgery Adjuvant Chemoimmunoradiotherapy