1. Federal Medical Center, Keffi
PATIENT CARD/E-FOLDER
Number: 20335666 Category: General
Name: JIBRIN SALIHA Phone No: 08142388189
Sex: Female Religion: Islam
Age: 14 Ethnic: HAUSA
Address: ANGWAN DADI KEFFI Next of Kin: FATIMA JIBRIN
3/1/2023 12:06 pm Notes RECORDED BY
MORNING DUTY REPOTY:
DIAGNOSIS: Newly Diagnosed Type 1 DM with Hyperglycaemia/gycosuria
IN/PT: A 13 year old girl admitted on the 30/12/2022. Being managed of the said diagnosis,
met off iv fuid
Vital signs not checked ( Pt not in bed)
Mother reassured and counselled about her babys condition
Patient G/C is fair
momoh constance divine @Paediatric Medical Ward PMW
RESULT DATE LAB RESULT PERFORMED BY
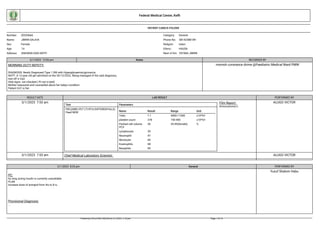
3/1/2023 7:53 am
Test Parameters
FBC((WBC/PLT CT/PCV/DIFFERENTIALS)
Paed NEW Name Result Range Unit
Twbc 7.1 4000-11000 x10^9/l
platelet count 278 150-400 x10^9/l
Packed cell volume
PCV
36 35-45(female) %
Lymphocyte 39
Neutrophil 47
Monocyte 06
Eosinophils 08
Basophils 00
Film Report:
Anisocytosis(+)
ALUGO VICTOR
3/1/2023 7:53 am Chief Medical Laboratory Scientist: ALUGO VICTOR
2/1/2023 8:33 pm General PERFORMED BY
PC:
As long acting insulin is currently unavailable
PLAN
Increase dose of actrapid from 4iu to 8 iu .
Provisional Diagnosis:
…
Yusuf Shalom Habu
Printed by UTAJI ONYI HELEN on 3/1/2023 2:10 pm Page 1 of 14
2. 2/1/2023 6:30 pm Notes RECORDED BY
EVENING DUTY:
DIAGNOSIS: Newly Diagnosed Type 1 DM with Hyperglycaemia/gycosuria
IN/PATIENT: A 13 year old Teenager admitted on the 30/12/2022. Being managed of the above diagnosis,
met off IVF
Vital signs checked and recorded
Due medication administerd short acting soluble insulin 4 IN at 6:00pm and there was no needle to administered long acting Glargine
patient and mother reassured and supported psychologically
Patient G/C is fair.
NRS. ROSELINE DANGIWA @Paediatric Medical Ward PMW
2/1/2023 10:36 am Notes RECORDED BY
NURSES NOTE:
MORNING DUTY
DIAGNOSIS: Newly Diagnosed Type 1 DM with Hyperglycaemia/gycosuria
IN/PT: A 13 year old girl admitted on the 30/12/2022. Being managed of the said diagnosis,
met off iv fluid and was eating with mum outside
Vital signs checked and recorded T-36.4*c ,P-78b/m and R-20c/m
Mother reassured and counselled about her babys condition
Patient G/C is fair.
Nrs. Babagambo Halima @Paediatric Medical Ward PMW
2/1/2023 10:30 am Notes RECORDED BY
null: Nrs. Babagambo Halima @Paediatric Medical Ward PMW
2/1/2023 10:23 am General PERFORMED BY
PC:
RWR(Dr Eke)
A 13year old female adolescent who was referred from GOPD yesterday on account of suspected Newly diagnosed DM patient with FBG of 20.3mmol/l. c/o
Excessive Urination x 1yr
Excessive eating x 1yr
At presentation FBG-20.3mmol/l
Being managed for 1. Diabetic mellitus 2. Gungivial hyperplasia ? Cause
Currently on
-Tabs Vit c
-Subcutaneous insulin (long and short acting)
Available investigations
HBAIc- 7.2 %,
Urinalysis-, glucose 2+, normal ketone,
EUCR-- essentially normal except for slight Hypercalcaemia 11.2mg/dl , HCO3-18.0mmo/l .
O/E
-Conscious, and alert,, afebrile(35.2*c), well hydrated, not cyanosed, nil pedal edema. Wt-36kg
Ht-1.07m
BMI=31.4kg/m"2
Tanner Stage 2 CVS
PR- 96bpm
BP- 100/70mmHg HS- S1&S2
Chest
RR- 18bpm
Equal chest expansion
Yusuf Shalom Habu
Printed by UTAJI ONYI HELEN on 3/1/2023 2:10 pm Page 2 of 14
3. VBS
Abd
FMWR
Nil abdominal tenderness
LOSOKO
CNS
Conscious, oriented in TPP
Pupils 4mm, round, reactive to light Nil neck stiffness
Tone normal in the limbs
ASS
1. Diabetic mellitus
2. Gungivial hyperplasia ? Cause
PLAN
-Ct Tab Vitamin C 200mg tds x 2/52
-Ct Subcutaneous Insulin therapy using short soluble Insulin ( Actrapid ) and long acting insulin Glargine.
-Give Short acting subcut Insulin (Actrapid ) 4IU 30mins pre breakfast,(6-7am ) lunch ( 2pm ) and Dinner ( 6pm ) then
-Give Long acting subcut Insulin ( Glargine ) 10IU by 8pm
- Advise parents to get Glucometer to monitor RBG before every meal , 2hrs post prandial and at bed time charted in an RBG CHART.
- Dietary counselling to reduce carbohydrate intake and optimize protein intake especially plant protein and vegetables.
-Monitor urine output and ensure adequate intake of at least 3L//day
-counsel parent on child’s condition , possible complications
Provisional Diagnosis:
…
2/1/2023 5:00 am Notes RECORDED BY
NURSES NOTE:
NIGHT DUTY REPORT:
DIAGNOSIS: Newly Diagnosed Type 1 DM with Hyperglycaemia/gycosuria
IN/PT: 13 year old girl admitted on the 30/12/2022 and managed for the above diagnosis
Patient was met sitting on bed on duty resumption
Vital signs checked and recorded T-37.3*c ,P-100b/m and R-24c/m
Has sub. insulin (Actrapid 4iu) administered at 6am
Patient ate after 30 minutes of injection
Mother reassured and counselled about her babys condition
Patient G/C is fair
NRS. JACOB STEPHENIE IVEREN @Paediatric Medical Ward PMW
1/1/2023 10:03 pm Notes RECORDED BY
NURSES NOTE:
B/P-80/60mmgh
NRS. JACOB STEPHENIE IVEREN @Paediatric Medical Ward PMW
1/1/2023 5:37 pm Notes RECORDED BY
EVENING DUTY:
DIAGNOSIS: Newly Diagnosed Type 1 DM with Hyperglycaemia/gycosuria
IN/PT: 13 year old girl admitted on the 30/12/2022 and managed for the above diagnosis
Patient was met sitting on bed on duty resumption
Vital signs checked and recorded T-36.3*c ,P-101b/m and R-24c/m
Chinyere Glory @Paediatric Medical Ward PMW
Printed by UTAJI ONYI HELEN on 3/1/2023 2:10 pm Page 3 of 14
4. Has sub. insulin (Actrapid 4iu) administered at 6pm
Patient ate after 30 minutes of injection
Mother reassured
Patient G/C is fair
1/1/2023 9:08 am Notes RECORDED BY
MORNING DUTY:
DIAGNOSIS: Newly Diagnosed Type 1 DM with Hyperglycaemia/gycosuria
IN/PT: 13 year old girl admitted on the 30/12/2022 and managed for the above diagnosis
Patient was met sitting on bed on duty resumption
Vital signs checked and recorded T-36.3*c ,P-100b/m and R-24c/m
Has sub. insulin (Actrapid 4iu) administered at 2pm
Patient ate after 30 minutes of injection
Mother reassured
Patient G/C is fair
NRS. AINA ELIZABETH ADUKE @Paediatric Medical Ward PMW
1/1/2023 6:13 am Notes RECORDED BY
MORNING DUTY:
DIAGNOSIS: Newly Diagnosed Type 1 DM with Hyperglycaemia/gycosuria
IN/PT: 13 year old girl admitted on the 30/12/2022 and managed for the above diagnosis
Patient was met sitting on bed on duty resumption
Vital signs checked and recorded T-36*c P-100b/m R-26c/m
RBS 10.9mmol/l at 5:55am
has sub. insulin (Actrapid 4iu) administered at 6am
Patient ate after 30 minutes of injection
Patient G/C is fair
Mother reassured
She was transfered to PMW
NRS. MERCY ARUWA @Emergency Paediatric Unit /Ward (EPUW)
1/1/2023 5:14 am Notes RECORDED BY
null:
DIAGNOSIS:Newly Diagnosed Type 1 DM with Hyperglycaemia/gycosuria
IN/PT: 13 year old girl admitted on the 30/12/2022 and managed for the above diagnosis
Patient was met sitting on bed on duty resumption
Vital signs checked and recorded T-36.2*c P-100b/m R-24c/m
RBS 10.9mmol/l at 5:55am
has sub. insulin (Actrapid 4iu) administered at 6am
Patient ate after 30 miin of injection
Patient G/C is fair
Mother reassured
NRS. AGBO IKOH @Ophthalmology GSRF service unit
31/12/2022 6:13 pm Notes RECORDED BY
EVENING DUTY:
DIAGNOSIS:Newly Diagnosed Type 1 DM with Hyperglycaemia/gycosuria
IN/PT: 13 year old girl admitted on the 30/12/2022 and managed for the above diagnosis
Patient was met sitting on bed on duty resumption
Vital signs checked and recorded T-36.2*c P-100b/m R-24c/m
has sub. insulin (Actrapid 4iu) administered at 6pm
Patient ate after 30 minit of injection
Patient G/C is fair
Mother reassured
Muhammed Sanni Habiba @Ophthalmology GSRF service unit
Printed by UTAJI ONYI HELEN on 3/1/2023 2:10 pm Page 4 of 14
5. 31/12/2022 2:09 pm General PERFORMED BY
PC:
EPU WWR - (Dr Emeh)
A 13year old female adolescent who was referred from GOPD yesterday on account of suspected Newly diagnosed DM patient with FBG of 20.3mmol/l.
c/o
Excessive Urination x 1yr
Excessive eating x 1yr
At presentation FBG-20.3mmol/l
Being managed for 1. Diabetic mellitus
2. Gungivial hyperplasia ? Cause
Currently on
-Tabs Vit c
-Subcutaneous insulin (long and short acting)
Available investigations
HBAIc- 7.2 %,
Urinalysis-, glucose 2+, normal ketone,
EUCR-- essentially normal except for slight Hypercalcaemia 11.2mg/dl , HCO3-18.0mmo/l .
O/E-Conscious, and alert,, afebrile(36.8*c), well hydrated, not cyanosed, nil pedal edema.
Wt-36kg
Ht-1.07m
BMI=31.4kg/m"2
Tanner Stage 2
CVS
PR- 102bpm
BP- 100/70mmHg
HS- S1&S2
Chest
RR- 16bpm
Equal chest expansion
VBS
Abd
FMWR
Nil abdominal tenderness
LOSOKO
CNS
Conscious, oriented in TPP
Pupils 4mm, round, reactive to light
Nil neck stiffness
Tone normal in the limbs
ASS
1. Diabetic mellitus
2. Gungivial hyperplasia ? Cause
PLAN
-Ct Tab Vitamin C 200mg tds x 2/52
-Ct Subcutaneous Insulin therapy using short soluble Insulin ( Actrapid ) and long acting insulin Glargine.
-Give Short acting subcut Insulin (Actrapid ) 4IU 30mins pre breakfast,(6-7am ) lunch ( 2pm ) and Dinner ( 6pm ) then
-Give Long acting subcut Insulin ( Glargine ) 10IU by 8pm
- Advice parents to get Glucometer to monitor RBG before every meal , 2hrs post prandial and at bed time charted in an RBG CHART.
- Dietary counselling to reduce carbohydrate intake and optimize protein intake especially plant protein and vegetables.
-Monitor urine output and ensure adequate intake of at least 3L//day
-Counsel parents on child"s condition , possible complications .
Dr. Oguaju Joy Chidinma
Printed by UTAJI ONYI HELEN on 3/1/2023 2:10 pm Page 5 of 14
6. Provisional Diagnosis:
…
31/12/2022 10:57 am Notes RECORDED BY
NURSES NOTE:
MORNING DUTY
DIAGNOSIS:Newly Diagnosed Type 1 DM with Hyperglycaemia/gycosuria
IN/PT: 13 year old girl admitted on the 30/12/2022 and managed for the above diagnosis
Patient was met sitting on bed on duty resumption
Vital signs checked and recorded T-36.2*c P-104b/m R-26c/m
FBS at 6:30am 18.4mmol/L, Insuline 8iu administered at 6:50 am
Patient ate her breakfast at 7:20am
Patient G/C is fair
Mother reassured
NRS. AYIMA HUSSEINI RABI @Ophthalmology GSRF service unit
31/12/2022 7:09 am General PERFORMED BY
Provisional Diagnosis:
…
Yusuf Shalom Habu
31/12/2022 7:09 am LABORATORY REQUESTS
Name Specimen Comment Raised By
FBC((WBC/PLT CT/PCV/DIFFERENTIALS) Paed NEW Blood Yusuf, Shalom Habu
urine m/c/s/ (child) Urine Yusuf, Shalom Habu
Urinalysis (Child) NEW Urine Yusuf, Shalom Habu
Other Informaion: null
31/12/2022 6:09 am Notes RECORDED BY
NIGHT DUTY REPORT:
DIAGNOSIS:Newly Diagnosed Type 1 DM with Hyperglycaemia/gycosuria
IN/PT: 13 year old girl admitted on the 30/12/2022 and managed for the above diagnosis
Patient was met sitting on bed on duty resumption
Vital signs checked and recorded T 36.2*c P 84b/m R 24c/m
FBS at 6:30am 18.4mmol/L, Insuline 8iu administered at 6:50 am
Patient ate her breakfast at 7:20am
Patient G/C is fair
Mother reassured
NRS. AGNES EDET LAWRENCE @Ophthalmology GSRF service unit
30/12/2022 10:47 pm General PERFORMED BY
PC:
A 13year old female adolescent born to Afor Muslim parents residing at Keffi Nasarawa state referred from GOPD on account of suspected Newly diagnosed DM patient with FBG of 20.3mmol/l.
c/o
Gwafan Kuyet
Printed by UTAJI ONYI HELEN on 3/1/2023 2:10 pm Page 6 of 14
7. Excessive Urination x 1yr
Excessive eating x 1yr
Child was in apparent state of health when she noticed excessive urination. She had an increased night time urination of 4 and daytime frequency of 5, compared to frequency of 2/0
No hx of pain on micturition, no change in colour, no urgency, no haematuria.
No history of facial swelling or ay other part of the body
There is also a history of excessive feeding described as increased frequency of meals from 3 times daily in premorbid state to 5 times daily when symptoms started.
Child also feels hungry immediately after eating a meal. but no weight gain
However there is mild weight loss , evidence by loose ftting of previously fitted clothes.
There is associated excessive thirst.
However no abdominal pain, no nausea, no vomiting, no passage of watery stools.
Mother is a known diabetic diagnosed at 29 years of age. On follow in DASH
At onset of illness, she was taken to GH Keffi, 3 months ago where she was diagnosed based on account of above symptoms and raised RBG , nutritional counselling was done, and no medications
given. With persistence of symptoms Child presented to GOPD samples taken for investigations at Alheri lab which showed the following -:
FBG - 20.3mmol/l , HBAIc- 7.2 %, Urinalysis-, glucose 2+, normal ketone,
EUCR-- essentially normal except for slight Hypercalcaemia 11.2mg/dl , HCO3-18.0mmo/l .
She was subsequently referred here for further management.
No past hx of admission , no blood transfusion or surgery in the past.
Genotype is unknown, no hx suggestive of scdx
A product of term gestation, pregnancy was booked at 4mo GA in this facility, Pregnancy went unevenful, carried to term delivered at home, cord was severed by a nurse, no neonatal complications
Was exclusively breast fed for 6mo, complimentary feeds introduced there after , and weaned off breast milk at 14mo
Fully immunized according to the NPI schedule
Detailes of when milestone was achieved cannot be remembered by the mother she however said milestones were achieved at same time as her other children
She is currently in Js 3 class , last position was 10th out of 24 students.
Child is the 4th out of 5 children in a mongamous family setting. Other Children are alive and doing well.
Father is 50yrs old mechanic while mother is a 40yrs old food trader. Both parents have 1LOE
They live in a 4bedroom flat
Source of drinking water is sachet water
Source of cooking fuel is firewood
Sleeps under ITN
ROS: essentially normal
Has no known drug allergy
O/E
Conscious, and alert,, afebrile(36.7*c), well hydrated, not cyanosed, nil pedal edema.
Wt-36kg
Ht-1.07m
BMI=31.4kg/m"2
Tanner Stage 2
CVS
PR- 80bpm
BP- 90/60mmHg
HS- S1&S2
Printed by UTAJI ONYI HELEN on 3/1/2023 2:10 pm Page 7 of 14
8. Chest
RR- 18bpm
Equal chest expansion
VBS
Abd
FMWR
Nil abdominal tenderness
LOSOKO
CNS
Conscious, oriented in TPP
Pupils 4mm, round, reactive to light
Nil neck stiffness
Tone normal in the limbs
ASS
1. Diabetic mellitus
Plan
Cont ongoing management
Provisional Diagnosis:
Dm
30/12/2022 9:53 pm General PERFORMED BY
PC:
Update (Discussed with Dr adebiyi)
As long acting insulin is currently unavailable
PLAN
Increase dose of actrapid from 4iu to 8 iu .
If rbs is less than 4 mmol/l .... allow food intake prior to insulin actrapid dose.
If rbs is greater than 4 mmol/ l, give insulin before food intake
Ensure postprandial rbs check.
Provisional Diagnosis:
Dm
Gwafan Kuyet
30/12/2022 7:10 pm General PERFORMED BY
Dr. Obinwa Chinonye Modesta
Printed by UTAJI ONYI HELEN on 3/1/2023 2:10 pm Page 8 of 14
9. PC:
PTOC- SR Review- Dr. Keji
A 13yr old JSS 3 student who was diagnosed as a diabetic pt 3 month ago at GH Keffi but yet to start medication. Complains of
Excessive eating x 1 year
Excessive thirst x 1 year
Excessive urination x 1 year
Gum enlargement x 6/12
Headache x 2/52
Excessive eating was noticed 1 year ago, described as increased frequency of meals from 3 times daily in premorbid state to 5 times daily when symptoms started.
Child also feels hungry immediately after eating a meal.
Excessive urination also started about a year ago, described as a change from three to five times urination during the day and from nil to four times night voiding. Nil painful urination. Nil bedwetting. Nil
incontinence. Nil blood in urine.
There is increased thirst necessitating pt waking up to drink at least twice at night.
Nil fever. Nil abdominal pains.
Gum enlargement was noticed 6 month ago by child's teacher and mother. Gum infiltrated between the teeth progressively but has been static in the last 2 month. Nil pain.
There is associated gum bleeding while sleeping on 2 occasions while brushing daily.
Nil mal odourious breath
Nil bleeding from any other part of the body.
Headache started 2/52 ago, frontal in location, mild in severity, usually occurred in the evening, dull in character.
Nil eye/ear ache. Nil double vision. Nil poor vision. Nil neck pain. Nil fever. Nil rash.
Nil history of abdominal trauma. Nil hx of mumps in childhood. Nil hx of abdominal surgery. Nil hx of exposure to pesticides/chemicals.
Mother is a known diabetic diagnosed at 29yrs and is on medication.
Nil previous hospital admission/nil blood transfusion.
There is hx of diabetes in mother's paternal uncle. Nil hx of recurrent boils or infection in pt.
No hx of similar symptoms in 6yr old and 22yr old female siblings and 28yr and 20yr old male siblings.
Since onset of ill health, child was initially taking herbal concoction from different herbalist at different times. Child stopped herbal concoction just a week ago.
Child presented at GH Keffi 3 month ago and was diagnosed to be diabetic and placed on dietary modification. Child then presented at GOPD a day ago and was referred here.
O/E
Conscious, active, afebrile, well hydrated, not cyanosed, nil pedal edema.
Tanner Stage 2
CVS
PR- 80bpm
BP- 90/60mmHg
HS- S1&S2
GIT
Gum hypertrophy
Good oral hygiene
Nil abdominal tenderness
LOSOKO
CNS
Conscious, oriented in TPP
Speech I'd coherent
Pupils 4mm, round, reactive to light
Nil neck stiffness
Tone normal in the limbs
Chest
RR- 18bpm
Printed by UTAJI ONYI HELEN on 3/1/2023 2:10 pm Page 9 of 14
10. VBS
ASS
1. Diabetic mellitus
2. Gungivial hyperplasia ? Cause
PLAN
- Tab Vitamin C 200mg tds x 2/52
- Ct earlier outlined management
- Retrieve pending investigation
- Counsel parents on diagnosis and prognosis
Provisional Diagnosis:
1. Diabetic mellitus
2. Gungivial hyperplasia ? Cause
30/12/2022 7:01 pm Notes RECORDED BY
EVENING DUTY:
ADMISSION NOTE
ASS- Newly Diagnosed Type 1 DM with Hyperglycaemia/gycosuria
NEW PT=13year old female adolescent born to Afor Muslim parents residing at Kef Nasarawa state referred from GOPD on account of suspected Newly diagnosed DM patient with FBG of 20.3mmol/l.
c/o Excessive Urination x 1yr
Excessive eating x 1yr
O/A/E O/E- Conscious, not in obvious distress, afebrile () , pale, anicteric , not cyanosed, not signifcant peripheral lympadenopathy, no pedal oedema.
Wt-36kg
P/M/S/HX Child was seen in GH Kef 3 months ago where she was diagnosed type 1 DM
F/S/HX =She is currently in Js 3 class , last position was 10th out of 24 students.
Child is the 4th out of 5 children in a mongamous family setting. Father is 50yrs old mechanic while mother is a 40yrs old food trader . parents have primary level of education.
They live in a 4bedroom flat.
NSG ACTIONS
child admitted and made comfortable on couch in consulting room
vital signs checked and recorded
-pt was Commenced on Subcutaneous Insulin therapy using short soluble Insulin ( Actrapid ) administered at 7/20pm.
-Give Short acting subcut Insulin (Actrapid ) 4IU 30mins pre breakfast,(6-7am ) lunch ( 2pm ) and Dinner ( 6pm ) then
-Give Long acting subcut Insulin ( Glargine ) 10IU by 8pm
child reassured
g/c is fair
Muhammed Sanni Habiba @Ophthalmology GSRF service unit
30/12/2022 5:36 pm General PERFORMED BY
PC:
Fasting Blood Glucose (29/12/2022)- 20.4 (3.9-6.0)mmol/l
HbA1C (29/12/2022)- 7.2 (<6)%
E/u/cr (29/12/2022)
Na- 138.6 (135-148)mmol/l
K- 4.5 (3.5-5.5)mmol/l
Cl- 98.5 (96-106)mmol/l
HCO3- 18.0 (21-33)mmol/l
Urea- 3.5 (1.9-8.3)mmol/l
Creatinine- 67.8 (40-106)umol/l
URINALYSIS (29/12/2022)
Dr. Obinwa Chinonye Modesta
Printed by UTAJI ONYI HELEN on 3/1/2023 2:10 pm Page 10 of 14
11. Appearance- Amber and slightly cloudy
pH- 6.0
Blood- Normal
Glucose- ++
Urobilinogen- Normal
Bilirubin- Normal
Protein- Normal
Nitrite- Normal
Ketone- Normal
Ascorbic Acid- Normal
Provisional Diagnosis:
..
30/12/2022 12:04 pm General PERFORMED BY
PC:
13year old female adolescent born to Afor Muslim parents residing at Keffi Nasarawa state referred from GOPD on account of suspected Newly diagnosed DM patient with FBG of 20.3mmol/l.
c/o Excessive Urination x 1yr
Excessive eating x 1yr
Child"s problem was noticed a year ago when she started going to pass urine more than usual times in the day , about 4 times per day and 4 times in the night as against D/N of 2/0 .there is associated
increase in volume of urine , no hx of nocturia, no dyuria.no hx of bedwetting.
There is hx of associated frequency of eating with large quantity of food intake now 5 times in a day.She feels nauseated but no hx of vomiting, abdominal pain or distension.No hx of weight loss but
appetite said to be good and eats much.
No history of headache, loss of consciousness or fainting episodes.
Mother is a diabetic been followed up at DASH.
Child was seen in GH Keffi 3 months ago where she was diagnosed based on account of above symptoms and RBG was done which as high but was given dietary counsel and was not placed on
medication . Child presented to GOPD yesterday on account of frequent urination necessitating samples taken for investigations at Alheri lab which showed the following -:
FBG - 20.3mmol/l , HBAIc- 7.2 %, Urinalysis-, glucose 2+, normal ketone,
EUCR-- essentially normal except for slight Hypercalcaemia 11.2mg/dl , HCO3-18.0mmo/l .
She was subsequently referred here for further management.
No past hx of admission , no blood transfusion or surgery in the past.Genotype is unknown, no hx suggestive of scdx.
Yet to achieve menarche.
Prenatal , natal ,post natal could not be ascertained as mother is not available .
She was adequately immunized for age.
She is currently in Js 3 class , last position was 10th out of 24 students.
Child is the 4th out of 5 children in a mongamous family setting. Father is 50yrs old mechanic while mother is a 40yrs old food trader . parents have primary level of education.
They live in a 4bedroom flat.
O/E- Conscious, not in obvious distress, afebrile () , pale, anicteric , not cyanosed, not significant peripheral lympadenopathy, no pedal oedema.
Wt-36kg
Ht-1.07m
BMI=31.4kg/m"2
CVS
PR- 108bpm NVR pulses
BP- 90/60mmHg sitting
HS- 1st and 2nd only
RESP
spo2- 97% in room air.
RR-21breaths/min
Trachea- central
DR. OGIDI J.P
Printed by UTAJI ONYI HELEN on 3/1/2023 2:10 pm Page 11 of 14
12. Equal chest expansion
Good air entry
VBS
ABD
Full,mwr, not tender
LoSoKo.
CNS
Conscious , oriented in TPP
No neck stiffness
Normal tone in the limbs
No signs of meningeal irritation
Repeat RBG- 19.6mmol/l @ 1pm
Urinalysis
Colour- amber
Appearance - clear
Glucose -++
PH-7.0
ASS- Newly Diagnosed Type 1 DM with Hyperglycaemia/gycosuria
PLAN
Reviewed with Dr Adebiyi/Akunegbu
Admit under Team D
-Commence Subcutaneous Insulin therapy using short soluble Insulin ( Actrapid ) and long acting insulin Glargine.
-Give Short acting subcut Insulin (Actrapid ) 4IU 30mins pre breakfast,(6-7am ) lunch ( 2pm ) and Dinner ( 6pm ) then
-Give Long acting subcut Insulin ( Glargine ) 10IU by 8pm
- Advice parents to get Glucometer to monitor RBG before every meal , 2hrs post prandial and at bed time charted in an RBG CHART.
- Dietary counselling to reduce carbohydrate intake and optimize protein intake especially plant protein and vegetables.
-Monitor urine output and ensure adequate intake of at least 3L//day
-Do FBC, Urine mcs, daily urinalysis
-Counsel parents on child"s condition , possible complications .
Provisional Diagnosis:
? Newly diagnosed Type DM
30/12/2022 11:03 am General PERFORMED BY
PC:
A 13 year old female JSS-3 Student of eminent royal crown academy, keffi. brought by father on follow up for T1-DM diagnosed ABOUT ONE-YEAR ago at general hospital keffi not yet on any drugs.
Complains of increased urinary frequency, polydipsia, polyphagia and recurrent generalised body weakness x 1 year.
said to be apparently well until about 1 year ago developed above complains
Nil dysuria, vomiting nor diarrhea, nil weight loss nor any other complain.
YET TO ATTAIN MENARCHE.
mother is a known diabetic on treatment- ? age of onset
RESULTS- HBA1C= 7.2%
DR OBELE YAKUBU ABALAKU
Printed by UTAJI ONYI HELEN on 3/1/2023 2:10 pm Page 12 of 14
13. FBG= 20.3mmol/l
Urinalysis= glucose (++)
O/E- CONSCIOUS CALM NOT PALE ANICTERIC ACYANOSED
PR- 100
HS- S1 S2
CHEST, ABD- NAD
CNS- NAD
Provisional Diagnosis:
T1DM WITH HYPERGLYCEMIA(FBG- 20.3mmol/l) YET TO START MEDICATIONS
Treatment Plan:
Counsel
Discuss with consultant- DR. ANIBASA
REFER TO EPU
30/12/2022 10:58 am Clinic Referral PERFORMED BY
Patient was referred from General Outpatient GOPD to Paediatric Endocrinology
Transfer Notes: T1DM WITH HYPERGLYCEMIA(FBG- 20.3mmol/l) YET TO START MEDICATIONS
DR OBELE YAKUBU ABALAKU
30/12/2022 8:18 am VITAL SIGNS PERFORMED BY
Temperature: 36.3 Respiratory Rate: 24 Pulse Rate: 112
Weight: 38 Height: null BMI: 0
Systolic B.P.: null Diastolic B.P.: null BSA: 0
Random Blood Sugar: null Fasting Blood Sugar: null
Oxygen Saturation: null Pain Score: null Urinalysis: null
Comment:
MOSHOOD ABDULRAHEEM
22/12/2022 8:47 am General PERFORMED BY
PC:
A 13 year old female. A known diabetic patient as diagnosed 4/12 ago at general hospital keffi.
Complains of increased urinary frequency and generalised body weakness x 1 year.
HPC:
There is associated polyphagia and polydipsia.
Patient has not been on medications but has been on dietary control.
There is family history of DM in her mother.
Clinical Examination:
O/E; GCS
DR. DANIEL FREEMAN
Printed by UTAJI ONYI HELEN on 3/1/2023 2:10 pm Page 13 of 14
14. PR: 104bpm.
WT: 32kg.
Provisional Diagnosis:
? Type 1 DM.
Treatment Plan:
Patient education.
Investigations.
Review with results.
22/12/2022 8:47 am LABORATORY REQUESTS
Name Specimen Comment Raised By
POCT-sugar test(FBS/RBS) Paed NEW Blood DR. DANIEL, FREEMAN
Glycated heamoglobin (HBA1C) NEW Blood DR. DANIEL, FREEMAN
E/U/Cr (children)(NEW) Blood DR. DANIEL, FREEMAN
Other Informaion: null
22/12/2022 8:36 am VITAL SIGNS PERFORMED BY
Temperature: 36.1 Respiratory Rate: 24 Pulse Rate: 104
Weight: 32 Height: null BMI: 0
Systolic B.P.: null Diastolic B.P.: null BSA: 0
Random Blood Sugar: null Fasting Blood Sugar: null
Oxygen Saturation: null Pain Score: null Urinalysis: null
Comment:
NRS. OMOLARA OBAMUWE GRACE
Printed by UTAJI ONYI HELEN on 3/1/2023 2:10 pm Page 14 of 14