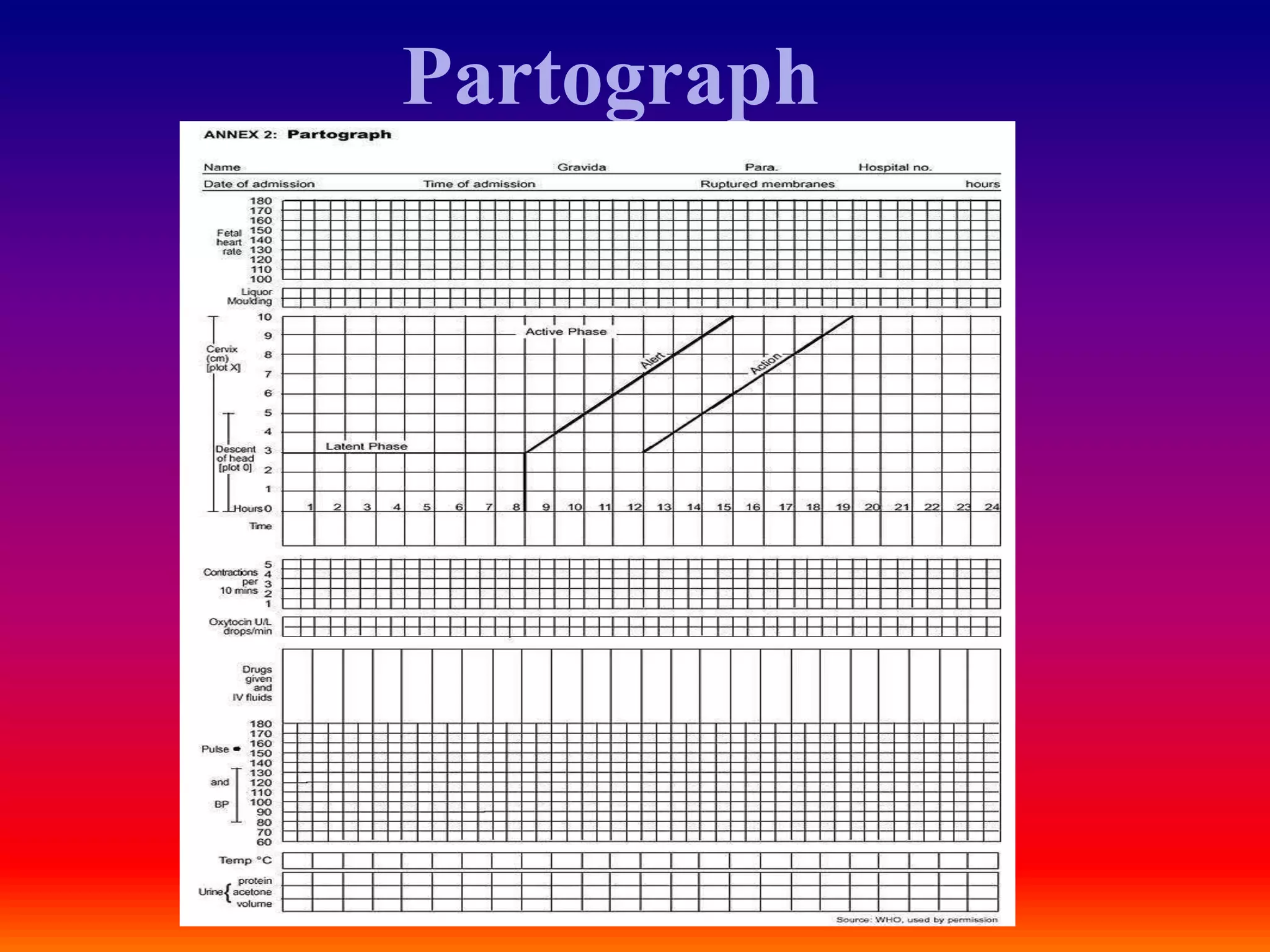
This document discusses the use of a partograph to monitor labor. A partograph is a graphical record used to monitor the progress of labor and assess the condition of the mother and fetus. It tracks cervical dilation, fetal descent, contractions and other metrics. Tracking these metrics against timelines helps identify abnormal labor progress. If progress deviates from alert or action lines, it warns of potential complications and need for intervention or transfer to higher level care. The partograph is a tool to manage labor but does not identify pre-existing risk factors. Its aim is early detection of problems to improve outcomes for mother and baby.