
Recommended
More Related Content
Similar to JAUNDICE.pptx
Similar to JAUNDICE.pptx (20)
Recently uploaded
Recently uploaded (20)
JAUNDICE.pptx
- 1. JAUNDICE
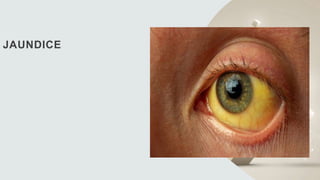
- 2. Introduction • Jaundice/ icterus, is a condition characterized by yellow discoloration of skin, conjunctivae, and mucus membranes as a result of widespread tissue deposition of the pigmented metabolite bilirubin. • Normal total bilirubin level <1-1.5mg/dl • Jaundice seen if Value exceeds 3mg/dl • Bilirubin have high affinity for elastin rich tissues eg sclera, frenulum of tongue,so jaundice appear first here .
- 3. Bilirubin metabolism bilirubin is the end product of heme Degradation
- 4. • Bilirubin uptake to be mediated by liver specific bilirubin transporter (BT) by facilitating diffusion process and by simple diffusion process • Intracelluar binding to S-glutathion transferase to keep bilirubin in solution • Conjugation with uridine diphosphate (UDP)-glucuronic acid done by the enzyme bilirubin UDP-glucuronosyl transferase(B-UGT1A1) into monoglucuronide,diglucuronide • Conjugated bilirubin transported into the bile canaliculus by an ATP-dependant export pump eg.MRP-2,ABCC2
- 5. • Conjugated bilirubin in intestine converted to Urobilinogen by bacterial action which undergo hepatic reuptake and partly renal elimination. • Small amount secreted across sinusoidal membrane by MRP-3,that undergo renal elimination and reuptake to hepatocyte by OAP1B1,OATP1B3
- 6. Differential diagnosis of jaundice 1. Isolated disorders of bilirubin metabolism- Unconjugated hyperbilirubinemia- • Increased bilirubin production- • Haemolysis • Ineffective erythropoiesis • Blood transfusion • Resorption of hematomas •Decreased hepatocellular uptake- • Drugs such as rifampicin • Various cholecystography contrast agents
- 7. •Decreased conjugation – • Gilbert’s syndrome, Crigler-Nazzer syndrome type1 and type2 • Physiological jaundice of newborn • Drugs such as indinavir, atazanavir Conjugated or mixed Hyperbilirubinemia- Dubin johnson syndrome, Rotor’s syndrome
- 8. 2.Liver diseases- a. Hepatocellular dysfunction – Acute or subacute hepatocellular injury – • Viral hepatitis • Hepatotoxins such as ethanol, acetaminophen ,isoniazid , phenytoin • Ischaemia such as in hypotension , vascular outflow obstruction • Metabolic disorders such as Wilson’s ds, Reye’s syndrome
- 9. Chronic hepatocellular disease - • Viral hepatitis • Alcoholic liver disease • Hepatotoxins such as ethanol , vinyl chloride , vitamin A • Autoimmune hepatitis • Metabolic disorders such as Hemochromatosis , Wilson's ds, NAFLD, a1-antitrypsin deficiency
- 10. b. Cholangiocytic injury- • Primary biliary cirrhosis • Graft-versus-host disease • Drugs such as erythromycin, trimetholrim-sulfamethxazole, • Cystic fibrosis
- 11. 3. Obstruction of the bile ducts • Choledocholithiasis • Primary sclerosing cholangitis • Post surgical strictures • Cholangiocarcinoma • Pancreatic cancer • Metastatic lymphadenopathy • Ampullary carcinoma • Pancreatitis
- 12. Diagnostic approach to jaundice When clues are evaluated in the context of the physical findings and routine laboratory tests , jaundice can be characterized correctly as obstructive or nonobstructive.
- 14. History • H/O biliary surgery , fever, abdominal pain in right upper quadrant= Biliary obstruction with cholangitis • C/O anorexia, malaise, myalgia With H/O a known infectious exposure, injection drug use ,prior transfusions of blood products= suggestive of viral hepatitis • Family H/O jaundice or liver disease= suggest hereditary hyperbilirubinaemia or genetic liver disease
- 15. Physical Examination • High fever and abdominal tenderness in RUQ=suggests cholangitis • Palpable abdominal mass= Neoplastic cause of obstructive jaundice • Silver coloured stool=Suggests ampullary neoplasms • Ascites , splenomegaly and prominent abdominal veins= Suggests cirrhosis • Abdominal scar in midline or RUQ=Prior biliary surgery
- 16. Essential laboratory studies in patient with jaundice 1. Serum total bilirubin, Direct bilirubin 2. Alkaline phosphatase (ALP) 3. AST/SGOT 4. ALT/SGPT 5. Complete blood count 6. Prothrombin time
- 17. Serum bilirubin • Bilirubin is found in two fractions- Unconjugated or indirect- Insoluble in water, bound to albumin Conjugated bilirubin – water soluble ,excreted by kidney • Normal value of total serum bilirubin -1-1.5 mg/dl • If the direct acting fraction is <15% of total ,the bilirubin can be considered to all be indirect.
- 18. Alkaline phosphatase (ALP) • Increases in biliary obstruction and intrahepatic cholestasis • Not a specific marker • Elevation more than 4 times of normal is significant • More specific markers for cholestasis are gamma glutamyl transpeptidase[GGT], 5’ Nucleotidase
- 19. Aminotransferase (ALT,AST) • ALT, Cytosolic enzyme found predominantly in hepatocytes • AST, Found in cytosol and mitochondria of parenchymal cells of liver • Normal serum concentrations –10-40 IU/L • Levels of upto 300 IU/L are nonspecific and may be found in any liver disorder • Level >1000 IU/L occur almost exclusively in disorders associated with extensive hepatocellular injury such as in viral hepatitis, ischaemic liver injury, toxins or drug induced liver injury.
- 20. • Predominantly elevation of serum aminotransferase activity in comparison with alkaline phosphatase activity suggests that jaundice is the result of intrinsic hepatocellular disease • Pattern of the aminotransferase elevation can be helpful diagnostically AST:ALT Ratio <1 is suggestive of chronic viral hepatitis and NAFLD AST:ALT Ratio >2 is highly suggestive of alcoholic liver disease
- 21. Complete blood count • Leucocytosis= Suggests Biliary tract obstruction or other inflammatory disorders • Anaemia = Suggests haemolysis is the cause of bilirubin overload • Thrombocytopenia=. Characteristic finding in cirrhosis results from reduced platelet production from decrease hepatocyte synthesis of thrombopoietin or from increase of platelet consumption from splenic sequestration
- 22. Prothrombin time • Measure the plasma activities of coagulation factor 1,2,5,7,10 each of which is synthesized by hepatocytes • Prolongation of PT(and an associated increase in INR) can result from impaired hepatic synthesis of these proteins and from deficiency of vitamin K which is required as a cofactor for essential posttranslational modification of factor 2,7,9,10.
- 23. Efficient absorption of vitamin K by the small intestine requires an intact enterohepatic circulation of bile salts(hence ,an unobstructed biliary tree). Exogenous administration of vitamin K will generally normalize a prolonged PT in patients with Obstructive jaundice and intrahepatic cholestasis but not in patients with liver disease caused by hepatocellular injury.
- 24. Algorithm for evaluation and management
- 25. References 1.Harrison’s principles of internal medicine 2.Sleisenger and fordtran’s gastrointestinal and liver disease
- 26. Thank you