Call Now ☎ 9549551166 || Call Girls in Dehradun Escort Service Dehradun
07_1_Menstrual cycle.pptx
1. 27-1
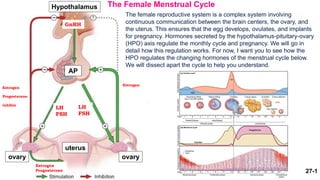
The Female Menstrual Cycle
The female reproductive system is a complex system involving
continuous communication between the brain centers, the ovary, and
the uterus. This ensures that the egg develops, ovulates, and implants
for pregnancy. Hormones secreted by the hypothalamus-pituitary-ovary
(HPO) axis regulate the monthly cycle and pregnancy. We will go in
detail how this regulation works. For now, I want you to see how the
HPO regulates the changing hormones of the menstrual cycle below.
We will dissect apart the cycle to help you understand.
Hypothalamus
GnRH
AP
ovary ovary
uterus
LH
FSH
LH
FSH
Estrogen
Progesterone
Estrogen
Progesterone
inhibin
Estrogen
2. The length of the menstrual cycle varies from woman to woman. The average cycle is every 28 days, but 21 to 40
days, are normal.
The Hypothalamus and the Pituitary
The hypothalamus release gonadotropin releasing hormone, GnRH. GnRH stimulates the anterior pituitary gland to
produce follicle stimulating hormone (FSH), the hormone responsible for follicle development and causing the level of
estrogen to rise. Luteinizing hormone (LH), the other reproductive pituitary hormone, aids in egg maturation and
provides the hormonal trigger to cause ovulation and the release of eggs from the ovary.
The Female Menstrual Cycle
Graph of
Hormones
made by the
anterior
pituitary
(gonadotropins =
FSH and LH)
FSH and LH cycles through the menstrual cycle. FSH is high when follicles need to develop. LH is the same level
during non-ovulation days. LH surges during ovulation on day 14 in a 28 day cycle.
3. 27-3
The Ovary
The main function of the ovaries is the production of eggs and hormones. As the levels of FSH and LH in the blood
increase with puberty, the eggs begin to develop. The follicles will start to make estrogen when it develops into the
secondary follicle stage. When the follicle reaches maturity, LH will stimulate ovulation. After Ovulation, the oocyte is
in the fallopian tube. The remaining follicle will form the corpus luteum and secrete estrogen and progesterone. If
implantation and pregnancy occurs, the corpus luteum will remain and support the pregnancy. If implantation does not
occur and the corpus luteum will shrivel to form the corpus albicans and die. The cycle will repeat itself and develop a
follicle and plan for implantation.
The Female Menstrual Cycle
Ovary response to
gonadotropins (FSH
and LH) leading to
follicular development
and ovulation Primary follicle Secondary follicle
mature follicle Ovulation Corpus luteum Corpus albicans
New follicles
4. 27-4
The Female Menstrual Cycle
The Uterus
The lining of the uterus, or endometrium, prepares each month for the implantation of an embryo. This preparation
occurs under the influence of estrogen and progesterone from the ovarian follicles. Estrogen promotes the growth of
the endometrial lining and progesterone thickens the lining for potential pregnancy. If no pregnancy develops,
estrogen and progesterone drops and the endometrium is shed as a menstrual period, about fourteen days after
ovulation.
Hormones
made by
the
ovary
Uterine
response to
the estrogen
and
progesterone
estrogen
progesterone
5. Hormonal chain of events
Anterior pituitary
Ovary - Follicle
Uterus
Hypothalamus
Hormones made by the anterior
pituitary (gonadotropins)
Hormones made by the
ovary
Ovary response to gonadotropin
Uterine response to the estrogen
and progesterone
6. Apply your knowledge
Hormone Produced by Target tissue Hormone action
GnRH (Gonadotropin
Releasing Hormone)
Hypothalamus Anterior Pituitary Stimulate the AP to produce
gonadotropins
FSH (Follicle Stimulating
hormone)
LH (Luteinizing Hormone)
Estrogen
Progesterone
Fill this chart about each of the reproductive hormones.
1. At what follicular developmental stage does the ovary start producing estrogen and progesterone?
2. At what follicular developmental stage does the ovary produce estrogen?
3. A female patient has very low FSH. What will happen with her follicular development?
4. Without follicular development, will the ovary produce estrogen?
5. If estrogen and progesterone does not drop and stays high, will there be a menstruation?
6. A female patient lacks LH surge, will she ovulate? Will she form a corpus luteum?
7. 27-7
The first day of menses (menstrual blood flow) is identified as cycle day one. Menstruation lasts for about 1-5 days.
Day 1-5 is called the Preantral Phase (for ovarian phase) and Menstrual Phase (for uterine phase).
Days 1-5: Preantral phase Explanation
Preantral Phase H-P-O axis Preantral Phase – We will begin the Hypothalamus-Ovarian
Axis at the ovary. The ovarian follicle has to communicate with the
brain about the status of its growth and readiness for ovulation. (1)
In the ovary the follicles are in the primary follicle stage and are
(2) not making much estrogen. (3) The low estrogen negative
feedback to the Hypothalamus and stimulate an (4) increase in
GnRH. (5) GnRH stimulate the pituitary to secretes more FSH. (6)
FSH stimulate the growth of several (15-20) follicles in the ovary.
One follicle will soon begin to grow faster than others. This is
called the dominant follicle and the preantral phase will end and
begin the next phase.
Menstrual Phase – The low estrogen does not support the
endometrium and the endometrium slough off. This is
menstruation and it will last 1-5 days.
8. In the ovary:
Preantral phase
FSH is high and stimulates follicle to develop. In
this phase the follicles have not formed an antrum
yet. That is why it is called pre-antral phase.
In the uterus:
Menstrual Phase
Preantral follicles makes very little estrogen.
Estrogen supports endometrium growth. With low
estrogen & progesterone, the endometrium is not
supported and will slough off.
Day 1 of menstruation
Lasts 1-5 days
Days 1-5: Pre-antral phase
Preantral phase
menstrual phase
Preantral phase
menstrual phase
9. 27-9
As the follicle grows from primary to secondary, one follicle will be come larger than all the others.
This is the dominant follicle. Cells in the dominant follicle develops and the antrum forms. The
secondary follicle will make more hormones. Blood levels of estrogen rise significantly by cycle day
seven.
Days 5-13: Antral phase
Antral phase – (1) in the ovary, the follicles are now in
the secondary phase with an antrum. (2) The follilcle
makes increasing amounts of estrogen. Progesterone is
not made until after ovulation by the corpus luteum. (3)
This higher estrogen negative feedback to the
Hypothalamus. (4) Hypothalamus makes lower GnRH. (5)
Lower GnRH will decrease the levels of FSH. (6) The fall in
FSH allows smaller (non-dominant) follicles to die off.
They are, in effect, "starved" of FSH. This allows for only
one dominant follicle to live. This is why most human
pregnancies only have one baby and twins are not
common.
Proliferative Phase – Increase in estrogen promotes the
growth of endometrium.
Antral H-P-O axis
10. In the ovary:
Antral phase
One dominant follicle develops antrum &
matures.
The dominant follicle produces estrogen.
Low FSH starves off the other smaller, non-
dominant follicles.
In the uterus:
Proliferative phase
Menstruation has ended. The increase in
estrogen from the dominant follicle
stimulates endometrium to proliferate.
Days 5-13: Antral phase
Antral phase
Proliferative phase
Antral phase
Proliferative phase
11. Antral Follicle Estrogen Production
1. LH from the AP binds to LH-
receptors on Theca Cells
2. LH stimulates theca cells to
produce testosterone.
3. Testosterone is bound by
granulosa cells. Testosterone should
not be released into the blood. The
proper amount of testosterone
production is important.
4. Testosterone is converted to
estrogen with the enzyme
aromatase.
5. Estrogen is released into the
blood.
1. A patient has elevated LH (3X higher than normal). How will this affect the level of testosterone
production? Will testosterone end up in the blood?
When the follicles are developed into
an antral follicle, the theca and
granulosa cells can make hormones.
12. 27-12
Ovulation: (1)The secondary follicle continue to grow
towards maturation. (2) The level of estrogen is
sufficiently high. (3) The HPO pathway will switch to
positive feedback. (4) The high levels of estrogen will
will stimulate the anterior pituitary to produces a sudden
sudden release of LH, usually around day thirteen of a 28
a 28 day cycle. (5) This LH peak triggers a complex set of
set of events within the follicles that result in the final
final maturation of the egg and egg extrusion from the
the ovary (Ovulation).
Days 14: Ovulation
H-P-O axis during Ovulation
13. Days 14: Ovulation
In the ovary:
Ovulation
The dominant follicle with high levels of estrogen
triggers an LH surge.
The LH surge leads to ovulation and the oocyte
exits the ovary and enters the fallopian tube.
In the uterus:
During Ovulation
The increasing levels of estrogen made by the
secondary follicle continue to grow the
endometrium.
Ovulation
Ovulation
14. The cells in the follicle that are left in the ovary after ovulation transforms to the corpus luteum. The corpus luteum
produce high amounts of estrogen and progesterone to prepare the lining of the uterus for implantation. If a pregnancy
occurs, the corpus luteum produces progesterone until ~10 weeks gestation. If no embryo implants, the circulating
levels of hormone decline with the degeneration of the corpus luteum and the formation of the corpus albicans.
Early and Mid-Luteal Phase
The luteal phase begins with ovulation and lasts
approximately 14 days. During the early, mid-luteal phase,
(1) the ovary has a corpus luteum. (2) it produces estrogen
and progesterone. (3) estrogen negative feedback to (4)
decrease GnRH and (5) decrease FSH. (6) Lower FSH
prevents the ovary from developing new follicles.
Day 15-24: Early and Mid-Luteal Phases
H-P-O axis for mid-luteal phase
Secretory Phase
The endometrial lining has been growing and continue to
grow with the presence of estrogen. With progesterone
present, the lining thickened and highly vascularized to
prepare for implantation of the fertilized egg.
15. In the ovary:
Early Mid-luteal Phase
Follicle without oocyte becomes corpus luteum
and produces progesterone & estrogen
In the uterus:
Secretory Phase
high progesterone stimulates glands to secrete
fluid => “bloated”
high estrogen stimulates proliferation of
endometrium
Day 15-24: Early and Mid-Luteal Phases
Early Mid-luteal Phase
Secretory Phase
Early Mid-luteal Phase
Secretory Phase
16. H-P-O axis for Late Luteal Phase
When no embryo implants, the circulating levels of hormone decline with the degeneration of the corpus
luteum and the formation of the corpus albicans. Corpus albicans do not make hormones and estrogen
and progesterone declines.
Day 25-28: Late Luteal Phase
Late-Luteal Phase
(1) In the ovary, the corpus luteum degenerates to form the
corpus albicans. (2) Estrogen and progesterone drops.
(3) negative feedback to the hypothalamus. (4) Low
estrogen brings GnRH up. (5) higher GnRH will stimulate
the anterior pituitary to increase FSH production. (6) high
FSH stimulate the ovary to develop a new set of follicles
thus starting a new cycle.
Premenstrual Phase
The degeneration of corpus luteum and the formation
of corpus albicans drops estrogen and progesterone.
Without estrogen and progesterone. The endometrium
is no longer supported. Oxygen is cut off and the
endometrial lining begins to die.
17. In the ovary:
Late Luteal Phase
Involution of corpus luteum causes estrogen &
progesterone to decrease
FSH rises and new follicles are primed
In the uterus:
Pre-menstrual Phase
Decrease in estrogen & progesterone cause
arteries to constrict. The lack of O2 & blood to
the endometrium leads to the tissue dying.
Day 25-28: Late Luteal Phase
Late luteal
Phase
Pre-menstrual Phase
Late luteal Phase
Pre-menstrual Phase
18. Apply your knowledge
1. How do low estrogen and progesterone levels affect levels of…
GnRH ____ FSH ____
2. Androgen is produced by __ cells with __ hormone stimulation. Androgen is converted to estrogen by __ cells.
3. Some women experience hormonal problems that result in low levels of FSH.
a) How would low FSH affect follicle development?
b) Will the patient ovulate? Menstruate?
4. A.J. carries a mutation in the BRCA1 gene and as a result has a 40-50% risk of developing ovarian cancer. To
decrease her risk, A.J. has her ovaries removed. How would the ovariectomy affect the levels of the following
hormones? Draw a HPO axis for this condition.
GnRH ____ FSH ____
estrogen ____
19. Polycystic Ovarian Syndrome
Polycystic ovary syndrome (PCOS) is an endocrine disorder that affects between 5-12% of women of reproductive
age, making it the most common hormonal disorder among women in this age group. Most often, symptoms first
appear in adolescence, around the start of menstruation. However, some women do not develop symptoms until their
early to mid-20's. Up to 10% of women are diagnosed with PCOS during gynecologic visits. Although PCOS presents
early in life, it persists through and beyond the reproductive years.
Three defining characteristics of PCOS:
1) Hyperandrogenisms (high androgen in the blood)
2) Oligo or amenorrhea (irregular or missing menstruation)
3) Polycystic ovaries (Cyst in the ovaries)
Must have hyperandrogenism AND oligo/amenorrhea to be diagnosed (NIH criteria)
The following characteristics are very often associated with PCOS, but not all are seen in every woman:
Hirsutism (excessive hair growth on the face, chest, abdomen, etc.); Hair loss (androgenic alopecia, in a classic "male
baldness" pattern); Acne; Polycystic ovaries; Obesity; Infertility or reduced fertility
Women with PCOS have a increased risk of developing the following health problems during their lives:
Insulin resistance; Diabetes; Lipid abnormalities; Obstructive sleep apnea; Cardiovascular disease; Endometrial
carcinoma (cancer)
20. 27-20
Pathophysiology of Polycystic Ovarian Syndrome Explanation of Next Figure
The exact cause of PCOS is not clear, but there is a link between genetics, obesity, and lack of activity
(1). Many women with PCOS have insulin resistance (2a) linked to obesity and sedentary lifestyle. A sign
of insulin resistance is (3) acanthosis nigricans, a skin disorder characterized by darkening
(hyperpigmentation) and thickening (hyperkeratosis) of the skin, occurring mainly in the folds (neck, armpit,
groin region)
Insulin resistance, obesity, low activity, and poor diet leads to Insulin levels increase (4) in the body and
may cause higher androgen levels (5). Higher levels of androgen leads to symptoms of (6) hirsutism
(face, back, chest and abdomen), acne, and alopecia (hair loss on the head).
Genetics, obesity, and lack of activity can also affect the LH:FSH ratio (2b). LH increases to 3 times or
more higher while FSH is low. The higher LH stimulates theca cells to produce higher levels of
androgen (5) and the androgen will end up in the blood causing symptoms observed (6). (7)The lower
FSH arrest follicles in the primary or early antral follicle stage and prevents follicles from developing
into maturity. Without a mature follicle, there is (8) no ovulation and the patient will experience infertility
(9). The follicles that remain in the ovary can form multiple cyst leading to polycystic ovary (10).
The developed follicle is what will produce estrogen and progesterone to grow and thicken the
endometrium. When the follicle becomes corpus albicans, the estrogen and progesterone drops and the
endometrium is shed. Without a follicular cycle, the endometrium does not grow or shed normally,
amenorrhea (11).
21. Genetics, Obesity, Sedentary lifestyle
Insulin Resistance
LH:FSH ratio
Insulin production
Androgen
Arrest in antral
follicle development
Anovulation Polycystic ovaries
Fertility Amenorrhea
Pathophysiology of Polycystic Ovarian Syndrome
Hirsutism, Acne,
& Alopecia
Acanthosis
nigricans
Abnormal feedback
from excess
androgen promotes
LH>>>FSH
22. Apply your knowledge
1. K.W. is 16 years old and has experienced oligomenorrhea (infrequent menstruation) for several years. Endocrine
screening shows she has high levels of free testosterone and a LH:FSH ratio of 3:1.
a) Is K.W. ovulating? How do you know?
b) Why is she not menstruating normally? How does her LH:FSH levels affect follicle development and
menstruation.
2. Ultrasound analysis shows K.W. has a number of ovarian follicular cysts. How do abnormal LH:FSH hormone levels
cause the formation of ovarian cysts?
3. K.W. has poor eating habits and a BMI (body mass index) that places her in the obese category. How could a poor
diet and obesity contribute to the development of PCOS?
4. K.W. has a darken ring of rough skin around her neck. What is this and what caused it?
5. Exercise, weight loss and better eating habits can decrease PCOS symptoms. How does these lifestyle changes
help with PCOS?