
Recommended
More Related Content
What's hot
Similar to CEMENTUM by Danish Hamid.pptx
Similar to CEMENTUM by Danish Hamid.pptx (20)
More from Danish Hamid
More from Danish Hamid (9)
Recently uploaded
Recently uploaded (20)
CEMENTUM by Danish Hamid.pptx
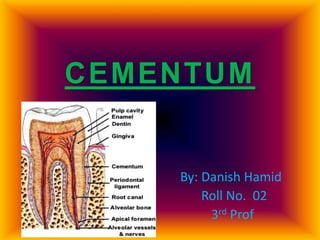
- 1. CEMENTUM By: Danish Hamid Roll No. 02 3rd Prof
- 2. Contents Introduction Physical Characteristics Chemical Composition Development Functions Types of Cementum Schroeder Classification Cementoenamel Junction Cementum Resorption and Repair Clinical Considerations
- 3. Introduction o Cementum is calcified, avascular mesenchymal tissue that forms the outer covering of the anatomical root. o It is part of the PERIODONTIUM. o It begins at cervical portion of the tooth and continues to apex.
- 4. Physical Characteristics o Pale yellow in color. o Lighter color, softer and more permeable than dentin. o Shows irregular surface. o Thickness ; – At coronal half:- 16 to 60 µm – At apical third & furcation area:- 150 to 200 µm
- 5. Chemical Composition Organic 50 – 55% Type I (90%)and Type III (5%) collagen fibers are embedded in ground substance. Proteins and Polysaccharides Inorganic 45 -50 % Hydroxyapatite Calcium Phosphorous Fluoride Water
- 6. Source of collagen fibers Extrinsic Fibers o Formed by fibroblasts. o Embedded portion of principal fibers of PDL. o Run in same direction of principal fiber o Also called Sharpey’s fibers. Intrinsic Fibers o Produced by cementoblasts. o Belong to cementum matrix. o Run parallel to root surface.
- 7. Development of Cementum o Rupture of Hertwig Root Sheath allows the mesenchymal cells of dental follicle to contact dentin where they start forming a continuous layer of cementoblasts. o Begins with deposition of irregular meshwork of collagen fibrils sparsely distributes in ground substance called pre-cementum or cementoid.
- 8. . o Followed by phase of matrix maturation, which subsequently mineralizes to form cementum. o Sometimes cementoblasts may get enclosed and trapped in the matrix, they are referred as cementocytes , and remain viable. o The formation of cementum is incremental , so we obtain Incremental lines of Salter.
- 10. Functions of cementum Primary function of cementum is anchorage that is by furnishing a medium for attachment of collagen fibres that bind the tooth to alveolar bone. Apical cementogenesis compensated for attrition of enamel, thereby maintaining functional occlusal relationship.
- 11. It serves as reparative tissue in case root fracture or resorption. It provides for fiber reattachment or relocation consequent to mesial drifting of teeth.
- 12. Types of cementum Cementum is of 2 two main types; Acellular and Cellular. 1. Acellular Cementum:- o It is the first cementum formed also known as Primary cementum. o It doesn’t contain cells. o It covers cervical third or half of the root.
- 13. . o It is formed before the root reaches the occlusal plane. o Sharpey’s fibers makeup most of structure and are inserted at rt. angles into root surface. o Thickness:- 30-230 µm.
- 14. 2. Cellular cementum:- o It is formed after the formation of Acellular cementum so called Secondary cementum. o It contains cells (Cementocytes) present in lacunae. o It covers apical third and inter-radicular region.
- 15. o It is formed after the tooth reaches the occlusal plane. o Sharpey’s fibers occupy smaller portions and are separated by other fibers arranges parallel to root surface.
- 16. Fig.;- Cellular and Acellular Cementum (with Cementocytes in lacunae)
- 17. Schroeder’s Classification This classification is based on location, morphology and histological appearance. 1. Acellular afibrillar cementum(AAC) 2. Acellular extrinsic fiber cementum(AEFC) 3. Cellular mixed stratified cementum(CMSC) 4. Cellular intrinsic fiber cementum(CIFC) 5. Intermediate cementum (The hyaline layer of Hope Well Smith)
- 18. Acellular Afibrillar Cementum (AAC) o It neither contains cells nor extrinsic or intrinsic collagen fibres. o It only contains mineralizes ground substance. o It is a product of cementoblasts and is found as coronal cementum. o Thickness: 1-15 µm
- 19. Acellular extrinsic fiber cementum (AEFC) o It is composed entirely of densely packed bundles of Sharpey fibres and lacks cells. o It is a product of fibroblasts and cementoblasts. o It is found in cervical third of root. o Thickness: 30-230 µm
- 20. Cellular Mixed Stratified Cementum (CMSC) o It is composed of extrinsic and intrinsic fibers and may contain cells. o It is a co product of fibroblasts and cementoblasts. o It appears in apical third of roots, apices and furcation areas. o Thickness: 100-1000 µm
- 21. Cellular Intrinsic Fiber Cementum (CIFC) o It is composed of intrinsic fibres and cells but no extrinsic fibers. o It is a product of cementoblasts. o It fills the resorption lacunae.
- 22. Intermediate cementum o It is an ill-defined zone near cemento-dentinal junction. o It contains cellular remnant of the Hertwig’s sheath embedded in calcified ground substance. o It contains enamel like proteins which help in attachment of cementum to dentin.
- 23. .
- 24. Cementoenamel junction Three types of relationships can occur at cemento- enamel junction. a. Overlapping:- In 60-65% of cases, cementum overlaps the enamel. It occurs when the enamel epithelium degenerates at cervical termination permitting connective tissue to come in contact with the enamel surface.
- 25. b. Touching:- In about 30% of cases, an edge to edge butt joint exists between enamel and cementum. c. Gapping :- In 5-10% of cases, the cementum and enamel fail to meet. It occurs when enamel epithelium at cervical portion is delays its separation from dentin.
- 27. Cementum Resorption and Repair o Cementum is less susceptible to resorption than bone under same pressure because of being avascular. o Average number of resorption areas per tooth is 3.5 and are located in apical third (76.8%), middle third (19.2%) and gingival third (40%).
- 28. o Caused by local or systemic factors. o Local conditions include trauma from occlusion, orthodontic movement pressure, cysts, periapical & periodontal diseases. o Systemic conditions include calcium deficiency, hyperthyroidism, hereditary fibrous osteodystrophy and Paget disease.
- 29. o Resorption areas appear as bay-like concavities. o Cementum resorption is not continuous and may alternate with periods of repair and deposition of new cementum. o The reparative and resorbed cementum are demarcated by an irregular reversal line.
- 30. . o The repair of cementum requires the presence of cementoblasts and viable connective tissue. o The reparative cementum is less mineralized and exhibits small calcifies globules. Anatomic repair:- outline is re-established. Functional repair:- little cementum is formed and rest is filled by alveolar bone.
- 31. Fig:- Cementum Resorption and Repair
- 32. Clinical considerations 1. Hypercementosis It is an age-related phenomenon and refers to prominent thickening of cementum. It may be localized to one tooth or affects entire dentition. Occurs as generalized thickening of cementum with nodular enlargement of apical third of root.
- 33. It appears as spike like excrescences, created either by coalescence of cementicles or calcification of PDL fibres at site of insertion into cementum. Roots appear thick with rounded apices. The causes can of hypercementosis can be: accelerated elongation of tooth, inflammation, tooth repair or Paget’s disease.
- 35. 2. Ankylosis oIt is the fusion of the cementum and the alveolar bone with obliteration of PDL. oIt results in resorption of the root and its gradual replacement by bony tissue. oIt occurs in case of cemental resorption, occlusal trauma, chronic periapical inflammation, reimplanted or embedded teeth.
- 36. . o Ankylosed teeth lack physiologic mobility of normal teeth and give dull, muffled metallic sound on percussion. o Physiological drifting and tooth eruption doesn’t occur. o Radiographically, blending of the bone with the root is apparent.
- 37. Fig:- Molars showing ankylosis Normal Ankylosis
- 38. 3. Cementicles o These are small areas of dystrophic calcified tissue, which lie free in the periodontal ligament of lateral and apical root areas. o They may be formed by calcification of epithelial rests, CT between Sharpey’s fibers, or thrombosed capillaries.
- 39. o They may be free in PDL or attached or embedded in cementum.
- 40. 4. Concrescence o It is the union of two or more fully formed teeth through cementum only. o It is a result of traumatic injury or crowding of teeth with resorption of interdental bone by which two roots come in contact and become fused by cementum deposition.
- 41. 5. Cemental Spurs o These are symmetrical spheres of cementum attached to root surface. o Found near cementoenamel junction. o These result from irregular deposition of cementum on the root. o Can’t be easily removed since they are hard dental tissue.
- 42. Bibliography o Newmann and Carranza’s Clinical Periodontology o Orban’s Oral Histology and Embryology o Shafer’s Textbook of Oral Pathology o Researchgate.net o Wikipedia.org o Slideshare.net