
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to ADJUSTABLE TONGUE CRIB.pptx
Similar to ADJUSTABLE TONGUE CRIB.pptx (20)
More from AshokKp4
More from AshokKp4 (20)
Recently uploaded
Recently uploaded (20)
ADJUSTABLE TONGUE CRIB.pptx
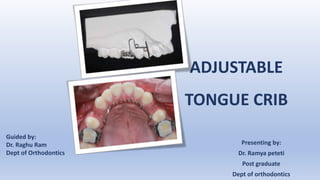
- 1. ADJUSTABLE TONGUE CRIB Presenting by: Dr. Ramya peteti Post graduate Dept of orthodontics Guided by: Dr. Raghu Ram Dept of Orthodontics
- 2. Introduction • Tongue thrust is an oral habit pattern related to the persistence of an infantile swallow pattern during childhood and adolescence, thereby producing an open bite and protrusion of the anterior teeth. • Deleterious habits such as thumb sucking and tongue thrusting play a major role in causing malocclusion, dental asymmetry and facial distortion (Meka and Suryadevara, 2015). A B
- 3. Classification of tongue thrusting: • Simple classification of Tongue thrust: Simple tongue thrust Complex tongue
- 4. • Type I: Non- deforming tongue thrust Classification by James S. Braner and Holt
- 5. • Type I: Non- deforming tongue thrust • Type II: Deforming anterior tongue thrust
- 6. • Type I: Non- deforming tongue thrust • Type II: Deforming anterior tongue thrust sub group 1: Anterior open bite
- 7. • Type I: Non- deforming tongue thrust • Type II: Deforming anterior tongue thrust sub group 1: Anterior open bite sub group 2: Anterior proclination
- 8. • Type I: Non- deforming tongue thrust • Type II: Deforming anterior tongue thrust sub group 1: Anterior open bite sub group 2: Anterior proclination sub group 3: Posterior crossbite
- 9. • Type III: Deforming lateral tongue thrust
- 10. • Type III: Deforming lateral tongue thrust sub group 1: Posterior open bite
- 11. • Type III: Deforming lateral tongue thrust sub group 1: Posterior open bite sub group 2: Posterior crossbite
- 12. • Type III: Deforming lateral tongue thrust sub group 1: Posterior open bite sub group 2: Posterior crossbite sub group 3: Deep overbite
- 13. • Type IV: Deforming anterior and lateral tongue thrust
- 14. • Type IV: Deforming anterior and lateral tongue thrust sub group 1: Anterior and posterior open bite
- 15. • Type IV: Deforming anterior and lateral tongue thrust sub group 1: Anterior and posterior open bite sub group 2: Anterior proclination
- 16. • Type IV: Deforming anterior and lateral tongue thrust sub group 1: Anterior and posterior open bite sub group 2: Anterior proclination sub group 3: Posterior crossbite
- 17. Treatment of tongue thrust: • Myofunctional exercises, • Fixed and removable appliances (cribs or rakes) (Singaraju and Kumar, 2009). A B C
- 18. • The tongue crib induces a change in the resting position of the tongue, thus allowing tooth eruption and closure of an anterior open bite.
- 19. • Most patients find it difficult to adapt and discontinue the treatment. A
- 20. • However, this is based on individual variation in the adaptive capacity of the tongue (Epker and Fish, 1977; Subtelny and Sakuda, 1964).
- 21. Fixed tongue loops (Veis and Christian, 2004) Tongue fence (Veis and Christian, 2004) Upper hay rake (Veis and Christian, 2004)
- 22. TADs Supported Tongue Crib: A New Minimalistic Design Journal of Contemporary Orthodontics, June 2018, Vol 2, Issue 2, (page 42-46)
- 23. Mittal R, Bapat SM, Garg N. Mittal bonded tongue thrusting appliance. APOS Trends Orthod 2014;4:139-40. Mittal bonded tongue thrusting appliance
- 24. • Modifications such as tongue crib with U-loops are commonly practised for multiple corrections (Abraham et al., 2013). • However, when these U-loops are adjusted, as a counter-effect, the height and angulation of the crib are altered. • To rectify these changes, counter-bends are given in the crib to place it in the desired position. • During these adjustments, the crib tends to break due to its rigid nature and acute bends. A B
- 25. • Hence, we came up with a modification to the conventional tongue crib which we call it as “adjustable tongue crib”, by incorporating helices at the acute bend areas, making them easy to adjust without fracture. • Most importantly, this design provides comfort to the patient through a gradual adaptation of the crib height and angulation. A B C
- 26. Fabrication A • 0.8-mm round hard stainless-steel wire
- 27. Fabrication A • 0.8-mm round hard stainless-steel wire • Universal plier
- 28. Fabrication • 3–4 cribs similar to a conventional tongue crib (canine to canine (Miller, 1969). A • 0.8-mm round hard stainless-steel wire • Universal plier
- 29. Fabrication • 3–4 cribs similar to a conventional tongue crib (canine to canine (Miller, 1969). • Anterior helices (inner diameter 3 mm) facing the occlusal side of the lateral cribs. A • 0.8-mm round hard stainless-steel wire • Universal plier
- 30. Fabrication • 3–4 cribs similar to a conventional tongue crib (canine to canine (Miller, 1969). • Anterior helices (inner diameter 3 mm) facing the occlusal side of the lateral cribs. • Adapt the connecting bar parallel to the lateral surface of the palate, 2mm away from the soft tissue. A • 0.8-mm round hard stainless-steel wire • Universal plier
- 31. Fabrication • 3–4 cribs similar to a conventional tongue crib (canine to canine (Miller, 1969). • Anterior helices (inner diameter 3 mm) facing the occlusal side of the lateral cribs. • Adapt the connecting bar parallel to the lateral surface of the palate, 2mm away from the soft tissue. • Posterior helices (inner diameter 3 mm) opposite to the occlusal side, 5mm before the lingual sheets. A • 0.8-mm round hard stainless-steel wire • Universal plier
- 32. Fabrication • 3–4 cribs similar to a conventional tongue crib (canine to canine (Miller, 1969). • Anterior helices (inner diameter 3 mm) facing the occlusal side of the lateral cribs. • Adapt the connecting bar parallel to the lateral surface of the palate, 2mm away from the soft tissue. • Posterior helices (inner diameter 3 mm) opposite to the occlusal side, 5mm before the lingual sheets. • U-loops (width x height = 5 x 7 mm) near the second premolar region. A • 0.8-mm round hard stainless-steel wire • Universal plier
- 33. Fabrication • 3–4 cribs similar to a conventional tongue crib (canine to canine (Miller, 1969). • Anterior helices (inner diameter 3 mm) facing the occlusal side of the lateral cribs. • Adapt the connecting bar parallel to the lateral surface of the palate, 2mm away from the soft tissue. • Posterior helices (inner diameter 3 mm) opposite to the occlusal side, 5mm before the lingual sheets. • U-loops (width x height = 5 x 7 mm) near the second premolar region. • Insert the distal extension into the lingual sheets and lock. A • 0.8-mm round hard stainless-steel wire • Universal plier
- 34. Change of Crib Position in the Anteroposterior Direction Compress the U-loop to retract the crib A
- 35. Change of Crib Position in the Anteroposterior Direction Compress the U-loop to retract the crib Expand the U-loop to protract the crib A B
- 36. A Change of Crib Position in the Vertical Direction Open the posterior helices to increase the height of the crib
- 37. A B Change of Crib Position in the Vertical Direction Open the posterior helices to increase the height of the crib Close the posterior helices to decrease the height of the crib
- 38. A Change of Crib Angulation Open the anterior helices for anti-clockwise rotation of the crib
- 39. A B Change of Crib Angulation Open the anterior helices for anti-clockwise rotation of the crib Close the anterior helices for the clockwise rotation of the crib
- 40. Advantages • The height, angulation and sagittal position of the crib can be adjusted as and when required. • Easy to adjust. • Easily adaptable by the patients. • Do not fracture during adjustments (due to the incorporation of helices).
- 41. B Case Application • Bidental proclination • Anterior open bite • Tongue thrusting habit • Adjustable semi-fixed tongue crib A
- 42. A B C D
- 43. A B C U-loops were compressed to retract the crib Posterior helices were closed to decrease the crib height Anterior helices were closed for a clockwise rotation of the crib angulation
- 44. Discussion • The tongue crib acts as a mechanical barrier against the thrusting tongue (Sayin et al., 2006). • Although the conventional tongue crib is rigid and restrains the tongue, it can not be easily repositioned in its angulation and vertical position (Abraham R et al., 2013). • Any attempt to adjust the position of the crib might lead to fracture. Moreover, the patients feel uncomfortable in the initial phase with the crib and will not cooperate with the treatment.
- 45. • With this modification, the patient’s discomfort level is initially reduced by positioning the crib in a convenient height and angulation (parallel to the axial inclination of maxillary anterior teeth and halfway to the overbite). • Once the patient gets adjusted with the appliance, the crib height and angulation are gradually adjusted to an ideal position in the subsequent visits. • The incorporation of helices in the appliance design to a certain extend would increase the flexibility of the overall appliance. • However, this aspect is countered by incorporating anterior helices opposite to the tongue force, which takes up the stress.
- 46. Conclusion Adjustable tongue crib is a patient-friendly appliance that is gradually adapted by adjusting the crib position without fracture.
- 47. References • Abraham R, Kamath G, Sodhi JS, Sodhi S, Rita C and Sai Kalyan S (2013) Habit breaking appliance for multiple corrections. Case Reports in Dentistry 2013: 647649. • Epker BN and Fish L (1977) Surgical-orthodontic correction of open bite deformity. American Journal of Orthodontics 71: 278–299. • Meka BP and Suryadevara S (2015) A simplified method of fabricating a habit breaking appliance. Journal of Clinical and Diagnostic Research 9: ZH01. • Miller H (1969) The early treatment of anterior open bite. International Journal of Orthodontics 7: 5–14. • Singaraju GS and Kumar C (2009) Tongue thrust habit - a review. Annals and Essences of Dentistry 1: 14–23. • Subtelny JD and Sakuda M (1964) Open bite: Diagnosis and treatment. American Journal of Orthodontics 50: 337–358.
- 48. Thank you…
Editor's Notes
- Retraction of anterior teeth will decrease the gap between the crib and the teeth, and sometimes the crib may even come into contact with the teeth, hindering further retraction of anterior teeth.
- Retraction of anterior teeth will decrease the gap between the crib and the teeth, and sometimes the crib may even come into contact with the teeth, hindering further retraction of anterior teeth.
- In severe open-bite conditions, incorporating a large sized (height) crib in the initial days of treatment will cause too much discomfort to the patient. Placing a comfortable height crib (approximately half the length of the open bite) in the initial days and gradually increasing the height by opening the posterior helices, makes it easy for the patient to adapt.
- In severe open-bite conditions, incorporating a large sized (height) crib in the initial days of treatment will cause too much discomfort to the patient. Placing a comfortable height crib (approximately half the length of the open bite) in the initial days and gradually increasing the height by opening the posterior helices, makes it easy for the patient to adapt.
- As the proclined anterior teeth come to normal axial inclination, crib angulation does not coordinate with the tooth inclination.
- As the proclined anterior teeth come to normal axial inclination, crib angulation does not coordinate with the tooth inclination.
- An adjustable semi-fixed tongue crib was delivered in a case with bidental proclination and anterior open bite due to tongue thrusting habit (Figure 5).
- (A) Initially, due to the severe anterior open bite, a comfortable crib height (approximately half the length of the open bite) was given. (B) Gradually, as the patient got adjusted to the appliance, the posterior helices were opened to increase the height of the crib, which occupied the full open bite. (C, D) Later, as the bite is closed, the height of the crib is reduced accordingly.
- Necessary adjustments were made to prevent contact of the crib with the teeth during the treatment progress due to tipping and retraction of the anterior teeth.