Protein Synthesis Inhibitors: Tetracycline, Chloramphenicol & Macrolides
•Download as PPT, PDF•
7 likes•3,921 views

Protein synthesis inhibitors it is the part of antimicrobial agents or Chemotherapy.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Protein Synthesis Inhibitors: Tetracycline, Chloramphenicol & Macrolides
Similar to Protein Synthesis Inhibitors: Tetracycline, Chloramphenicol & Macrolides (20)
More from Archita Srivastava
More from Archita Srivastava (15)
Recently uploaded
Recently uploaded (20)
Protein Synthesis Inhibitors: Tetracycline, Chloramphenicol & Macrolides
- 1. PROTIEN SYNTHESIS INHIBITORS Presented by – Archita srivastava M.pharm 1st year
- 2. CONTENT Protein synthesis Introduction of Protein synthesis inhibitors Pharmacology ofTetracycline Pharmacology of choramphenicol Pharmacology of Macrolides
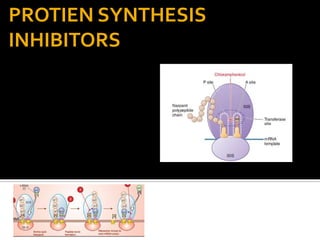
- 3. Protein synthesis Amino acids are shown as numbered circles. . In step 1, the charged tRNA unit carrying amino acid 6 binds to the acceptor site on the 70S ribosome. step 2.The peptidyl tRNA at the donor site, with amino acids 1 through 5, then binds the growing amino acid chain to amino acid step 3 The uncharged tRNA left at the donor site is released , and the new 6-amino acid chain with its tRNA shifts to the peptidyl site .
- 5. PROTEIN SYNTHESIS INHIBITOR Protein synthesis takes place on the ribosomes. Eukaryotic and prokaryotic ribosomes are different, and this provides the basis for the selective antimicrobial action of some antibiotics. The bacterial ribosome consists of a 50s subunit and a 30s subunit whereas in the mammalian ribosome the subunits are 60S and 40S . Bacteriostatic, protein-synthesis inhibitors that target the ribosome such as tetracycline and chloramphenicol, macrolides and ketolides, lincosamides (clindamycin), streptogramins (quinupristin/dalfopristin), oxazolidinones (linezolid),and aminocyclitols (spectinomycin).
- 6. TETRACYCLINE It is also called broad spectrum antibiotics. The tetracyclines are close congeners of polycyclic naphthacenecarboxamide. Tetracyclines are bacteriostatic antibiotics with activity against a wide range of aerobic and anaerobic gram- positive and gram-negative bacteria. Classification – 1.chlortetracycline 2. oxytetracyline 3. demeclocyline 4. Doxycycline 5.Minocycline
- 7. Mode of action It is bacteriostatic Inhibit protein synthesis. Bind to 30s ribosome.
- 8. PHARMACOKINETICS Absorption: All tetracyclines are adequately but incompletely absorbed after oral ingestion However, taking these drugs concomitantly with dairy foods in the diet decreases absorption due to the formation of nonabsorbable chelates of the tetracyclines with calcium ions. Distribution: The tetracyclines concentrate in the liver, kidney, spleen, and skin, and they bind to tissues undergoing calcification (for example, teeth and bones) or to tumors that have high calcium content All tetracyclines cross the placental barrier and concentrate in fetal bones and dentition.. ADMINISTRATIONAND FATE OFTETRACYCLINES.
- 9. Typical therapeutic applications of tetracyclines.
- 10. ADVERSE EFFECT
- 11. Resistance toTetracycline Resistance is primarily plasmid mediated and often inducible. The three main resistance mechanisms are Decreased accumulation of tetracycline as a result of either decreased antibiotic influx or acquisition of an energy- dependent efflux pathway; Production of a ribosomal protection protein that displaces tetracycline from its target, a “protection” that also may occur by mutation. Enzymatic inactivation of tetracyclines.
- 12. Chloramphenicol • Chloramphenicol, an antibiotic produced by Streptomyces venezuelae • It is a yellowish white crystalline solid, aqueous solution is quite stable, stands boiling, but needs protection from light. • The nitrobenzene moiety of chloramphenicol is probably responsible for the antibacterial activity as well as its intensely bitter taste. • Chloramphenicol is rapidly and completely absorbed from the gastrointestinal tract and is not affected by food ingestion or metal ions.
- 13. Mode of action Chloramphenicol inhibits bacterial protein synthesis by interfering with ‘transfer’ of the elongating peptide chain to the newly attached aminoacyl-tRNA at the ribosome- mRNA complex. It specifically attaches to the 50S ribosome near the acceptor (A) site and prevents peptide bond formation between the newly attached aminoacid and the nascent peptide chain
- 14. PHARMACOKINETICS DRUG INTERACTION. ADMINISTRATION AND FATE OF CHLORAMPHENICOL.
- 15. Resistance to Chloramphenicol. Resistance to chloramphenicol usually is caused by a plasmid- encoded acetyltransferase that inactivates the drug. Resistance also can result from decreased permeability and from ribosomal mutation. Acetylated derivatives of chloramphenicol fail to bind to bacterial ribosomes.
- 16. ADVERSE EFFECT Gray baby syndrome
- 17. CLINICAL USE Chloramphenicol is used topically in the treatment of eye infections because of its broad spectrum and its penetration of ocular tissues and the aqueous humor. It is ineffective for chlamydial infections. Chloramphenicol remains a major treatment of typhoid and paratyphoid fever in developing countries.
- 19. MACROLIDES The macrolides are a group of closely related compounds characterized by a macrocyclic lactone ring (usually containing 14 or 16 atoms) to which deoxy sugars are attached. Erythromycin was discovered in 1952 by McGuire and coworkers in the metabolic products of a strain of Streptomyces erythreus. Clarithromycin and azithromycin are semisynthetic derivatives of erythromycin.
- 20. Antimicrobial Activity. Erythromycin usually is bacteriostatic but may be bactericidal in high concentrations against susceptible organisms. The antibiotic is most active in vitro against aerobic gram-positive cocci and bacilli Staphylococci are considered susceptible at ≤0.5 μg/mL and streptococci at ≤0.25 μg/mL. In addition, Campylobacter, Legionella, Branhamella catarrhalis, Gardnerella vaginalis and Mycoplasma, that are not affected by penicillin, are highly sensitive to erythromycin
- 21. MODE OF ACTION Macrolides bind to the 50S ribosomal subunit of bacteria but not to the 80S mammalian ribosome; this accounts for its selective toxicity. Binding to the ribosome occurs at a site near peptidyltransferase, with a resultant inhibition of translocation, peptide bond formation, and release of oligopeptidyl tRNA.
- 22. Pharmacokinetics Erythromycin base is acid labile. To protect it from gastric acid, it is given as enteric coated tablets, from which absorption is incomplete and food delays absorption by retarding gastric emptying. Its acid stable esters are better absorbed. Erythromycin is widely distributed in the body, enters cells and into abscesses, crosses serous membranes and placenta, but not bloodbrainbarrier.
- 23. ADVERSE EFFECT AND DRUG INTEERACTION
- 24. Typical therapeutic applications of macrolides. • Erythromycin: This drug is effective against many of the same organisms as penicillin G therefore, it is used in patients who are allergic to the penicillins. • Atypical pneumonia caused by Mycoplasma pneumoniae: rate of recovery is hastened. • Whooping cough: a 1–2 week course of erythromycin is the most effective treatment for eradicating
- 25. REFERENCES 1. The pharmacological basis of therapeutics – Goodman & Gillman’s 12th edition page no. 1521-1545. 2. Basic and clinical pharmacology by katzung B. G 12th edition page no. 810-845. 3. K.D Tripathi , Essential of medical pharmacology 7th edition page no. 733 4. Lippincott’s Illustrated review , Pharmacology 4th edition page no. 596-613. 5. Modern Pharmacology with clinical applications Charles R. Craig Robert E. Stitzel 5th edition page no. 550-556