The effectiveness of peer educators and guidance counselling teachers to the ...
SPH Research Day Poster
1. In 1951, India became the first country in the developing world to
adopt a state-sponsored family planning program. Yet six decades of
family planning promotion, reproductive health outcomes in India
remain poor, particularly in the North.
The use of non-permanent contraceptive methods for spacing births is
particularly important in improving infant and maternal health (WHO,
2005). Internationally agreed human rights relevant to contraceptive
knowledge and services include the rights to information, education,
and the highest attainable standard of health (United Nations, 1966).
Studies have demonstrated that improvements in quality of care
according to these principles increases contraceptive use
(Cottingham, 2012). Moreover, the right to the highest attainable
standard of health obligates governments to ensure that contraceptive
services are of good quality (United Nations, 2000).
In 1997, India’s national program adopted a broader human rights
framework involving a focus on family planning needs, client choice,
and service quality (Visaria et al, 1999). Despite this official paradigm
shift, female sterilization remains the predominant form of
contraceptive use in India, with limited use of non-permanent
contraceptive methods for spacing births.
This research uses Socio-Ecological Model as its theoretical
framework to investigate determinants of non-permanent
contraceptive use among women living in rural Uttar Pradesh, India.
Semi-structured in-depth interviews were conducted with currently
married women aged 19-49 from June-August 2012.
All interviews were conducted in Hindi and were audio-recorded.
Interviews were transcribed, translated into English, and accuracy
checked. Initial coding was done by hand while the researchers were
in the field. A code book is currently being developed and coding will
be carried out using qualitative analysis software.
The methodology for data analysis is rooted in concepts of grounded
theory and constant comparison (Glaser and Strauss, 1967; Charmaz,
2006).
This study was approved by the University of California, Berkeley
Institutional Review Board, protocol 2012-02-4053.
• World Health Organization. Report of a WHO technical consultation on
birth spacing. Geneva, Switzerland: World Health Organization. 2005.
• United Nations. International covenant on economic, social and cultural
rights. New York: United Nations. 1966.
• Cottingham J, Germain A, & Hunt P. Use of human rights to meet the
unmet need for family planning. Lancet: 380(9837):172-80. 2012.
• United Nations Committee on Economic, Social, and Cultural Rights.
General comment 14: the rights to the highest attainable standard of
health. Geneva: United Nations. 2000.
• VisariaL, Jejeebhoy S, & Merrick T. From family planning to reproductive
health: challenges facing India. Int Fam Plan Per; 25(2 Suppl):S44-9.
1999.
BACKGROUND
Determinants of Non-Permanent Contraceptive Use
among Women in Rural Uttar Pradesh, India
Courtney E. Henderson, MPH, Anne Villumsen, Malcolm Potts, MB, BChir, FRCOG
METHODS
RESULTS
CONCLUSIONS
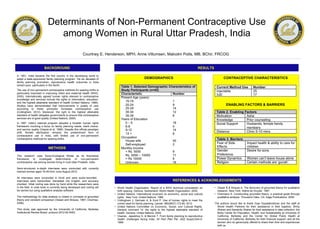
DEMOGRAPHICS
REFERENCES & ACKNOWLEDGEMENTS
• Glaser B & Strauss A. The discovery of grounded theory for qualitative
research. New York: Aldine de Gruyter. 1967.
• Charmanz K. Constructing grounded theory: a practical guide through
qualitative analysis. Thousand Oaks, CA: Sage Publications. 2006.
The authors would like to thank Gopi Gopalakrishnan and the staff at
World Health Partners for their assistance in field logistics; Shrity
Sharan and Sanskrity Sharan for their assistance in data collection; the
Bixby Center for Population, Health, and Sustainability at University of
California, Berkeley and the Center for Global Public Health at
University of California, Berkeley for their financial support; and all the
women who so generously offered to share their time and experiences
with us.
CONTRACEPTIVE CHARACTERISTICS
ENABLING FACTORS & BARRIERS