
Recommended
More Related Content
Similar to ASandler_DKA topic discussion.docx
Similar to ASandler_DKA topic discussion.docx (20)
More from AnnaSandler4
More from AnnaSandler4 (19)
Recently uploaded
Recently uploaded (20)
ASandler_DKA topic discussion.docx
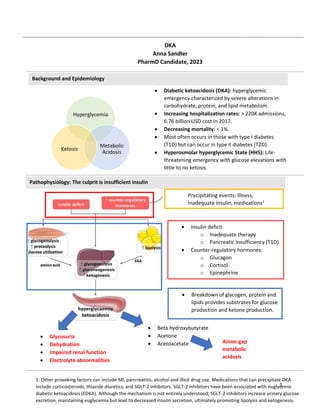
- 1. 1 Hyperglycemia Metabolic Acidosis Ketosis Background and Epidemiology Pathophysiology: The culprit is insufficient insulin DKA Anna Sandler PharmD Candidate, 2023 Diabetic ketoacidosis (DKA): hyperglycemic emergency characterized by severe alterations in carbohydrate, protein, and lipid metabolism. Increasing hospitalization rates: > 220K admissions, 6.76 billion USD cost in 2017. Decreasing mortality: < 1%. Most often occurs in those with type I diabetes (T1D) but can occur in type II diabetes (T2D). Hyperosmolar hyperglycemic State (HHS): Life- threatening emergency with glucose elevations with little to no ketosis. Insulin deficit o Inadequate therapy o Pancreatic insufficiency (T1D) Counter-regulatory hormones: o Glucagon o Cortisol o Epinephrine Precipitating events: Illness, inadequate insulin, medications1 Breakdown of glycogen, protein and lipids provides substrates for glucose production and ketone production. Anion-gap metabolic acidosis Glycosuria Dehydration Impaired renal function Electrolyte abnormalities 1: Other provoking factors can include MI, pancreatitis, alcohol and illicit drug use. Medications that can precipitate DKA include corticosteroids, thiazide diuretics, and SGLT-2 inhibitors. SGLT-2 inhibitors have been associated with euglycemic diabetic ketoacidosis (EDKA). Although the mechanism is not entirely understood, SGLT-2 inhibitors increase urinary glucose excretion, maintaining euglycemia but lead to decreased insulin secretion, ultimately promoting lipolysis and ketogenesis. Beta hydroxybutyrate Acetone Acetoacetate
- 2. 2 Mild Moderate Severe HHS Plasma glucose (mg/dL) >250 >250 >250 > 600 Arterial pH 7.25-7.30 7.00-7.24 <7.00 > 7.30 Serum Bicarbonate (mEq/L) 15-18 10-<15 <10 >18 Urine Ketones Pos. Pos. Pos. Small Serum Ketones Pos. Pos. Pos. </= small Anion gap >10 >12 >12 Variable Mental status Alert Alert/drowsy Stupor/coma Stupor/coma CBC With differential2 ABGs UA Ketones CMP EKG Gluc- ose Diagnosis and Presentation: A starvation of cells Presentation: A starved state Increased thirst, urination, hunger Volume depletion: Decreased skin turgor, dry mucosa, tachycardia, hypotension (severe) Fatigue, Weakness, alteration in mental status Signs of ketosis: Fruity breath odor Treatment: General Overview Severity of DKA is INDEPENDENT of glucose values! ABGs: Arterial Blood Gases; CBC: Complete blood count; CMP: complete metabolic pan; EKG: electrocardiogram; UA: Urine Analysis 2: Elevated white blood cell counts (10,000-15,000 mm3 ) are common in DKA and can occur due to dehydration, stress and movement of leukocytes away from the blood vessel walls. Do not forget: Correct serum Na and K extracellular shift Electrolytes Fluids Insulin Treated as a medical emergency Key themes (The 3Rs): Resuscitate, Replete, Reverse the gap SubQ Insulin
- 3. 3 Agent Dose/Rate Pearls NaCl Hypovolemic shock: infuse 0.9% NaCl as quickly as possible Hypovolemia without shock: 15-20 mL/kg lean body weight/hour for first couple of hours Euvolemia: Rate guided by clinical assessment Monitor urine output, blood pressure, and electrolytes As the patient stabilizes, the rate can be lowered to 4-14 mL/kg/hour or 250-500 mL/hour Once corrected Na is normal (> 135 mEq/L), the solution can be changed to 0.45% NaCl K KCl dose < 3.3 mEq/L 20-40 mEq/hour HOLD insulin 3.3-5.3 mEq/L 20-30 mEq added to each liter of IV replacement fluid > 5.3 mEq/L Delay KCl until K < 5.3 mEq/L Treatment: Fluids Fluids Benefits o Expand extracellular volume and help correct acidosis o Increase insulin responsiveness o Reduce stress hormone levels Agent of choice: 0.9% NaCl o Lack of strong evidence in support of balanced crystalloids3 Fluid composition dependent on electrolyte needs of the patient Treatment: Electrolyte replenishment It is important to achieve goal K levels since insulin will lead to an intracellular shift of K Almost all DKA patients have a K deficit usually due to glucose osmotic diuresis. Goal: 4-5 mEq/L Agent: IV potassium chloride (KCl), added to replacement fluid o Added to either isotonic or ½ NS depending on hydration, Na, and clinical assessment of the patient Electrolytes 3: A 2022 meta-analysis demonstrated that resuscitation with balanced crystalloids (e.g., Lactated Ringer’s) may result in shorter time to DKA resolution and shorter hospital stay compared to saline. A 2021 cluster, crossover open-label, randomized controlled phase 2 trial (SCOPE-DKA) conducted in seven Australian ICUs over 13 months revealed Plasmalyte- 148 may lead to faster metabolic acidosis resolution when compared to 0.9% NaCl. Additional subgroup analyses of balanced crystalloids in ED and ICU patients also demonstrate potential benefits over saline.
- 4. 4 Blood glucose Insulin rate >250 mg/dL 0.1 units/kg IV bolus followed by 0.1 units/kg/hour Alternative: 0.14 units/kg 200-250 mg/dL 0.02-0.05 units/kg/hr followed by dextrose-containing IV fluids until resolution of DKA Diagnosis SubQ Insulin regimen Prior diagnosis Resume outpatient dose New diagnosis Basel-bolus regimen (glargine/detemir/degludec- lispro/aspart/glulisine) Initial dose: 0.5 units/kg/day o Half basal, half bolus divided between meals Alternative: Insulin NPH HCO3 >/= 15 Clinical Stability Resoln pH > 7.3 PO feeding Anion gap </= 12 Transitioning to subcutaneous insulin Treatment: Insulin and Dextrose Insulin Agent: Insulin Regular (IV) Administered until anion gap is closed. Benefits: Reduces hepatic glucose production, inhibits ketogenesis and glucagon secretion. Resolution of DKA: Glucose < 200 mg/dL + any two of the following on the left Start when DKA has resolved and the patient is able to tolerate oral feeding. Continue IV insulin infusion for 2 hours after starting subcutaneous insulin. Dose dependent on prior or new diagnosis of diabetes. SubQ Insulin
- 5. 5 Honorable mention: Sodium Bicarbonate Use controversial and lack of prospective randomized control trials Patients who may benefit from cautious administration: o arterial pH </= 6.9 Dose: 100 mEq in 400 mL sterile water administered over two hours o Potentially life-threatening hyperkalemia Bicarbonate shifts K into cells Potential harmful effects: o Post-metabolic alkalosis once metabolic acidosis is resolved Metabolism of ketoacids generates bicarbonate o Reduction in hyper ventilatory drive leading to increased CO2 diffusion into the brain and paradoxical drop in cerebral pH o Recall, insulin is used to reverse the metabolic acidosis
- 6. 6 1. Self WH, Evans CS, Jenkins CA, et al. Clinical Effects of Balanced Crystalloids vs Saline in Adults With Diabetic Ketoacidosis: A Subgroup Analysis of Cluster Randomized Clinical Trials. JAMA Netw Open. 2020;3(11):e2024596. doi:10.1001/jamanetworkopen.2020.24596 2. Emmett M, Hirsch IB. Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults: Treatment. UpToDate. Published online March 24, 2022. 3. Westerberg DP. Diabetic ketoacidosis: evaluation and treatment. Am Fam Physician. 2013;87(5):337- 346. 4. Eledrisi MS, Elzouki AN. Management of Diabetic Ketoacidosis in Adults: A Narrative Review. Saudi J Med Med Sci. 2020;8(3):165-173. doi:10.4103/sjmms.sjmms_478_19 5. Alghamdi NA, Major P, Chaudhuri D, et al. Saline Compared to Balanced Crystalloid in Patients With Diabetic Ketoacidosis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Critical Care Explorations. 2022;4(1):e0613. doi:10.1097/CCE.0000000000000613 6. Ramanan M, Attokaran A, Murray L, et al. Sodium chloride or Plasmalyte-148 evaluation in severe diabetic ketoacidosis (SCOPE-DKA): a cluster, crossover, randomized, controlled trial. Intensive Care Med. 2021;47(11):1248-1257. doi:10.1007/s00134-021-06480-5 Picture links https://www.researchgate.net/figure/Pathogenesis-of-diabetic-ketoacidosis_fig1_341485181 https://www.pinterest.com/pin/6-symptoms-of-diabetic-ketoacidosis--201465783322879033/ http://clipart-library.com/closed-door-cliparts.html https://www.diabetes.co.uk/insulin/diabetes-and-injecting-insulin.html References
- 7. 7