Comprehensive Guide to Left Ventricular Noncompaction (LVNC
•Download as PPTX, PDF•
12 likes•1,055 views

lvnc diagnosis and implications for a pediatric cardiologist

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Comprehensive Guide to Left Ventricular Noncompaction (LVNC
Similar to Comprehensive Guide to Left Ventricular Noncompaction (LVNC (20)
More from Adhi Arya
More from Adhi Arya (9)
Recently uploaded
Recently uploaded (20)
Comprehensive Guide to Left Ventricular Noncompaction (LVNC
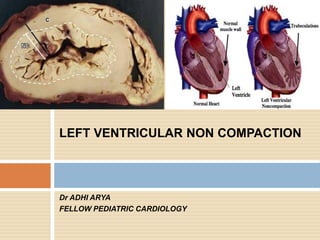
- 1. Dr ADHI ARYA FELLOW PEDIATRIC CARDIOLOGY LEFT VENTRICULAR NON COMPACTION
- 2. WHAT LVNC IS HISTORY PREVELANCE ETIOLOGY DIAGNOSIS DIFFERENTIAL DAIGNOSIS MANAGEMENT SUMMARY
- 3. WHAT IS LVNC Debate-Whether distinct cardiomyopathy or a morphologic trait shared by different types of cardiomyopathies or a normal morphological trait AHA- genetic cardiomyopathy ESC/WHO classifies LVNC as an unclassified cardiomyopathy
- 4. CARDIOMYOPATHY 1980 WHO defined cardiomyopathies as "heart muscle diseases of unknown cause" to distinguish cardiomyopathy from cardiac dysfunction due to known cardiovascular entities such as hypertension, ischemic heart disease, or valvular disease
- 5. 1995 WHO/ISFC expanded the classification -to take into consideration etiology as well as the dominant pathophysiology. Cardiomyopathies were defined as "diseases of the myocardium associated with cardiac dysfunction." classified according to anatomy and physiology into the following types, ●Dilated cardiomyopathy (DCM) ●Hypertrophic cardiomyopathy (HCM) ●Restrictive cardiomyopathy (RCM) ●Arrhythmogenic right ventricular cardiomyopathy/dysplasia (ARVC/D) ●Unclassified cardiomyopathies
- 6. The AHA(2006) and ESC (2008) classification systems differ from the earlier WHO/ISFC classification in emphasizing the distinction between familial and nonfamilial/non-genetic causes of cardiomyopathy excluding heart disease secondary to coronary artery disease, valvular, or congenital heart disorders. The ESC classification differs from the AHA classification in also excluding ion channelopathies.
- 7. The MOGE(S) classification for a phenotype- genotype-based nomenclature of cardiomyopathy was endorsed by the World Heart Federation -2013 was inspired by the TNM staging of malignant tumors and does not include ion channelopathies. The clinical applicability of this system has not yet been defined Five attributes:
- 8. ● MORPHOFUNCTIONAL (M) notation indicates a descriptive phenotypic diagnosis (eg, MD = dilated cardiomyopathy). ●THE ORGAN INVOLVEMENT (O) notation indicates if heart and/or extracardiac involvement is present (eg, OH+K = heart and kidney involvement). ●The GENETIC OR FAMILIAL INHERITANCE (G) notation indicates the nature of genetic transmission (eg, GAD = autosomal dominant). ●The ETIOLOGICAL ANNOTATION (E) provides description of the specific cause (eg, the specific gene and mutation as in EG- MYH7[p.Arg403Glu]). ●The addition of a FUNCTIONAL STATUS (S) term is considered optional (eg, SC-II = stage C disease in New York Heart Association functional class II).
- 11. HISTORY Spongy appearance of the myocardium first described by Grant in 1926 Engberding and Bender made the first clinical recognition with two-dimensional (2D) echocardiography in 1984
- 12. PREVALANCE true prevalence –unclear 9% of all pediatric cardiomyopathies 3 rd most common cardiomyopathy ( DCM/HCM) reported in 0.014–0.05% of adults( prevalence in patients undergoing echocardiography) Among CHF patients 3-4%. Probably an underestimate due to increased awareness these days and better echocardiograhic and MRI diagnosis
- 13. ETIOLOGY LVNC can originate during embryonic development or acquired later in life.
- 14. NONEMBRYOGENIC HYPOTHESIS. hypothesis that the pathogenetic mechanisms leading to noncompaction or increased trabeculation may occur in adult life, leading to acquired LVNC. particular phenotypic characteristics ofLVNC are identified in cases including pregnancy, sickle cell anemia, and athletes.
- 15. EMBRYOGENIC HYPOTHESIS. LVNC is thought to be caused by an arrest in the normal process of myocardial compaction.
- 16. Developmental considerations- development of the myocardial architecture which passes through four distinct steps (i) early heart tube (ii) emergence of trabeculations (iii) trabecular remodeling (iv) development of the multilayered spiral system Emergence of trabeculations and trabecular remodeling are the key steps to understand LVNC
- 17. Trabecular remodeling- remodelling starts after completion of ventricular septation at 8 weeks of gestation in human. Increase in ventricular volumes results in compression of the trabeculations with an increase in the thickness of the compacted myocardium. compaction process coincides with the invasion of epicardial coronary arteries and vascularization of the myocardium
- 18. Process progresses from- epicardium to the endocardium base to the apex septum to the free wall in the LV more in LV than right ventricle time of arrest of normal embryonic myocardial maturation determines the severity and extension of LVNC 18
- 20. GENETICS
- 21. Sporadic and familial form. AD more common than X-linked inheritance Familial recurrence between 18 and 50% Mutations in the G4.5 gene on Xq28 resulting Barth syndrome with DCM and LVNC in a pediatric population.
- 22. DIAGNOSIS ECHO( Chin/Jenni/stollberger) CONTRAST ECHO DE-MRI ADVANTAGES AND LIMITATIONS OF EACH PITFALLS THAT CAN LEAD TO MISDIAGNOSIS OF LVNC
- 24. 24
- 30. In these cases, contrast-enhanced echocardiography can better show trabeculations because contrast medium diffuses into the intertrabecular recesses that communicate with the ventricular cavity
- 31. LIMITATIONS OF ECHO operator dependent the apex, most frequently affected, can be difficult to visualize during echocardiography a double-layered myocardium or trabeculations may not be clearly visualized at echocardiography Misdiagnosis as another type of cardiomyopathy, such as hypertrophic cardiomyopathy short-axis images may not be perpendicular to the LV long axis and can produce the morphologic appearance of prominent trabeculations that mimic LVNC
- 32. Preferred views / end-systole vs end diastole Papillary muscles are easier to exclude in short axis which could look as trabeculations in 4c view End systole because differentiation between compacted and non compacted layers is difficult in end diastole
- 33. HCM shares morphological features with LVNC, but prognosis and treatment strategies differ between LVNC and HCM Homogeneously reduced LV function in LVNC, as opposed to preserved apical and more reduced basal function in HCM which may represent specific differences in embryogenesis and pathogenesis in the two cardiomyopathies. LVNC patients had increased number of trabeculations, thinner MWT, and lower EF compared to HCM patients and assessment of these parameters may help to characterize LVNC in patients with overlapping phenotypes.
- 34. CARDIAC MRI
- 35. ECHO DIAGNOSIS
- 37. DE MRI In LVNC, areas of trabecular and subendocardial delayed contrast enhancement can be appreciated and are related to the presence of subendocardial and trabecular fibrosis and fibroelastosis
- 38. ADVANTAGES OF MRI 3D approach-allows imaging of the entire volume of the heart with lower investigator dependency Better delineation of trabeculations and affords more accurate and reliable evaluation of the extent of noncompacted myocardium than does 2D echocardiography cardiac MRI has potential in the detection of segmental noncompaction in any area of the LV wall.
- 39. The right ventricle is better visualized with cardiac MRI than with echocardiography, and concomitant right ventricular noncompaction may be better identified. Delayed enhancement imaging can depict myocardial fibrotic foci that represent the substrate for potentially lethal arrhythmias Delayed enhancement also can be useful in the differential diagnosis from apical thrombus and endomyocardial fibrosis
- 40. LIMITATIONS OF MRI Higher cost, long acquisition times, and limited availability patient with pace makers
- 41. Approach to trabeculations detected on 2D ECHO
- 42. D/D DCM HCM MYOCARDITIS
- 43. Clinical features 3 main manifestations Congestive heart failure Arrythmias Thromboembolism Findings vary among patients, ranging from asymptomatic left ventricular dysfunction to severe, disabling congestive heart failure.
- 44. Both systolic and diastolic ventricular dysfunction have been described. Restrictive hemodynamics by cardiac catheterization, Initial presentation as a restrictive cardiomyopathy,
- 45. Heart Failure Diastolic Systolic Pathophysiology Abnormal relaxation Decreased compliance due to volume of trabeculations Subendocardial hypoperfusion chronic microvascular ischemia No significant epicardial coronary disease
- 46. Differences in pediatric population Ventricular arrythmias Sudden death Thromboemblic events are rare as compared to adult population
- 47. Patient characteristics in different studies
- 48. MANAGEMENT No specific treatment available Family members of proband should be screened using ECHO Genetic testing may useful in identifying familial forms Anticoagulation-(INR 2-3) 1. Decreased systolic function with EF below 40% 2. History of thromboembolism 3. Atrial fibrillation 49
- 49. ICD/biventricular pacing- no robust data available for guideline indication for device therapy as per current guideline.
- 50. Summary
- 51. THANK YOU
Editor's Notes
- Definition of cardiomyopathy- PRIMARY( predominantly heart)—genetic(HCM/ARVCLVNC/Mch ) /mixed (DCM/RCM)or aquired( myocarditis/stress induced TAKASUBO/peripartum IDM) SECONDARY ( other system involvement)
- In clinical practice, however, the term "cardiomyopathy" has also been applied to diseases of known cardiovascular cause (eg, “ischemic cardiomyopathy” and “hypertensive cardiomyopathy”).
- In a population-based retrospective cohort study of primary cardiomyopathies in Australian children isolated LVNC accounted for 9.2% of all cases and was identified as the third most frequent cardiomyopathy after dilated and hypertrophic cardiomyopathies. This prevalence was very similar to that seen in the Texas Children’s Hospital echocardiography database (9.5%)
- These act as foci for arrythmias
- Black blood and cine SSFP images must be compared to avoid incorrect diagnosis
- Diastolic dysfunction in ventricular noncompaction may be related to both abnormal relaxation and restrictive filling caused by the numerous prominent trabeculae. The origin of systolic dysfunction in noncompaction is unclear, but a body of evidence is accumulating that points toward subendocardial hypoperfusion and microcirculatory dysfunction playing roles in ventricular dysfunction and arrhythmogenesis.