
Recommended
Recommended
More Related Content
Similar to Finance and Accounting Management and PlanningChapter O.docx
Similar to Finance and Accounting Management and PlanningChapter O.docx (20)
More from AKHIL969626
More from AKHIL969626 (20)
Recently uploaded
Recently uploaded (20)
Finance and Accounting Management and PlanningChapter O.docx
- 1. Finance and Accounting Management and Planning Chapter Objectives After reading this chapter, you should be able to 1. Describe the essence of financial governance and working capital policy. 2. Apply the functions of long-term finance to management in the healthcare industry. 3. Explain the essence of accounting as it applies to healthcare management. 6 © Imagebroker.net/SuperStock Finance and Accounting Management and Planning Chapter 6 The relationships among the practices of medicine, healthcare management, and finan- cial management can easily be described as being complex. A physician in an individual practice, one in a group of specialists, and managers within a larger healthcare facility setting all encounter myriad challenges associated with setting prices for services; receiving payments
- 2. from insurance companies, patients, and the government; paying for medical equipment and supplies; and covering the costs of operation, including wages for support staff, the price of a physical office space through a lease or a purchase, and other expenses. Meanwhile, healthcare managers must also contend with requests for purchases of new equipment, increased space, and a variety of additional items that may or may not be suited to a healthcare organization’s goals. Healthcare managers also oversee payroll, billing statements, accounts payable and receivable, third-party reimbursements, discounting systems, tax statements and bills, and numerous finan- cial and accounting activities. All of these tasks relate to the process of cash flow management, or working capital policy. Working capital policy poses challenges for managers in every type of industry. However, health- care providers face additional obstacles that most private-sector companies do not. For example, any physician or pharmacy accepting Medicare and Medicaid patients often encounters diffi- culties in receiving reimbursements in a timely fashion. The dilemma follows a com- mon cycle: A patient receives care or fills a prescription; reimbursement documents are filed with the appropriate government agency; then the wait begins, many times for months. Meanwhile, supply bills, sala- ries, utilities, and other expenses come due and must be paid. Thus, any pharmacy or medical practice that accepts Medicare or Medicaid but that does not have a substan-
- 3. tial cash reserve has a problem. Consider the dilemma of Dr. Madalene Green, a solo practitioner at Potomac Arthritis and Rheumatism in Bethesda, Maryland. Medicare covers 50% of her patients. In a recent government entangle- ment over budget issues, Medicare stopped making payments. The net result was that Dr. Green had to forgo her own salary in order to remain solvent (Washington Business Journal, 2010). In 2008, physicians in California and other Western states complained that they were owed mil- lions of dollars in backlogged Medicare reimbursements. This continuing problem has led some physicians to turn away elderly patients and has pushed others to near bankruptcy. Doctors who serve high numbers of Medicare patients say they have been forced to default on rent, lay off staff, and plead with drug suppliers to continue shipments of medicines (Yoshino, 2008). The expansion of the government’s role in managing the healthcare system has led many to worry that these types of problems will only continue to increase. With physicians who try to © Keith Brofsky/Digital Vision/Thinkstock ▲▲ Many medical providers must wait a long time before receiving government payments for products and services.
- 4. Financial Governance and Working Capital Policy Chapter 6 establish practices lacking cash reserves, and with other organizations at the brink of default due to such payment delays, many have called on Congress to become involved and help resolve these problems. This chapter examines the natures of finance and accounting as they apply to the field of health- care. The first section outlines the forms, methods, and analyses used in managing an orga- nization’s financial system and presents working capital policy, which directs the oversight of day-to-day operations. Next, the chapter discusses pricing issues and the types of financial instruments that organizations may use to accomplish an organization’s longer-term goals. The final section describes the role of accounting in a healthcare organization’s operations. 6.1 Financial Governance and Working Capital Policy Financial governance in the field of healthcare involves two primary responsibilities: (1) over- sight of day-to-day operations that require financing and (2) planning for and implementing financial instruments that provide for the organization’s long- term financial needs (Gapenski, 2003). Tending to a healthcare provider’s financial well-being constitutes a primary concern for managers in the healthcare system. The increasing complexity of the economic and politi- cal environments in the area of finance makes this task highly demanding. Rigorous track- ing of an organization’s financial activities constitutes one crucial component in managing this
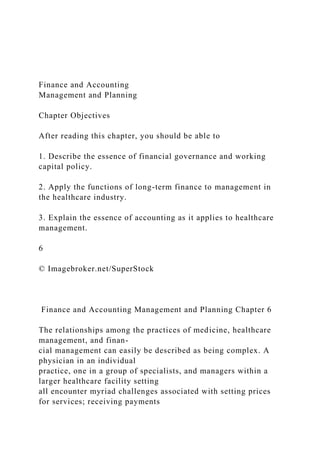
- 5. complexity. Financial Documents and Statements Finance and accounting departments prepare several documents and statements that assist healthcare managers in overseeing the organization’s monetary well-being. Three forms that assist the finance and accounting departments, as well as other organizational leaders, include a balance sheet, an income summary, and a ratio analysis. Balance Sheet A balance sheet summarizes an organization’s current status with regard to assets, liabilities, and equity. Figure 6.1 presents the items located in each portion of a balance sheet. Note that an organization’s total assets may be divided into what it owes (total liabilities) and what it owns (total equity) as follows: Total assets = Total liabilities + Total equity Balance sheets are typically prepared on an annual basis. The balance sheet provides a financial manager with a snapshot of the organization’s current position in terms of debt and equity. When managers examine a series of balance sheets that have been prepared over several years, they can study trends regarding growth of assets, changes in levels of liability, and differences in levels of equity in order to determine the organization’s financial well-being over time (Weygandt, 2013).
- 6. Financial Governance and Working Capital Policy Chapter 6 Income Summary An income summary is an accounting or financial statement that provides a somewhat different purpose for a profit-seeking organization than it does for a nonprofit. Managers in nonprofit, or not-for-profit, providers use an income summary to make sure that revenues exceed expenses. In a nonprofit, the manager works to make sure that organizational funds (the amount by which rev- enues exceed expenses) are being used wisely and efficiently, with sufficient monies to subsidize other goals, such as support of the less fortunate in the community and the expansion of medical services over time. A manager in a for-profit hospital, however, wishes to understand whether annual operations do indeed result in profits to be retained in order to build share value growth or to be distributed as dividends to shareholders. Figure 6.2 displays the elements of a standard income summary. Figure 6.1 Elements in a balance sheet f06.01_HCA340.ai Assets Liabilities Equity Short-term assets Cash Marketable securites
- 7. Accounts receivable Inventory Short-term liabilities Accounts payable Payments due trade credit commercial paper Common stock Paid-in surplus Preferred stock Retained earnings Long-term assets Building Equipment Financial instruments Long-term liabilities Loans Bonds
- 8. Lease payments Assets Liabilities Equity Short-term assets Cash Marketable securites Accounts receivable Inventory $2,750,000 1,250,000 3,750,000 250,000 Short-term liabilities Accounts payable Payments due trade credit
- 9. commercial paper $ 500,000 1,250,000 750,000 250,000 Common stock Paid-in surplus Preferred stock Retained earnings $9,000,000 3,000,000 0 $6, 250,000 Total short-term assets $8,000,000 Total short-term liabilities $2,750,000 Long-term assets
- 10. Building Equipment Financial instruments $20,000,000 10,000,000 0 Long-term liabilities Loans Bonds Lease payments $ 1,500,000 15,000,000 50,000 Total long-term assets $30,000,000 Total long-term liabilities $17,000,000
- 11. Total assets $38,000,000 Total liabilities $19,750,000 Total equity $18,250,000 Financial Governance and Working Capital Policy Chapter 6 Healthcare organizations receive revenues from multiple sources, including patients, insur- ance providers, and government payments for services. As Figure 6.2 shows, these revenues are totaled. For a healthcare organization, the cost of goods sold portion of an income summary includes the total expenses for medical supplies and other items directly related to the delivery of health services. Depreciation is tallied for all buildings and equipment, and a healthcare man- ager may use several different methods to depreciate an asset over time. Unusual expenses may include a settlement of a lawsuit or other nonroutine payments, while unusual income includes any gifts or bequeaths that the organization receives. Note that taxes are paid only by profit-seek- ing health organizations. Thus, net income after taxes (NIAT) is the bottom-line profit earned by these organizations (Finney, 2012). However, the government does not charge nonprofit organiza- tions, such as many skilled nursing facilities, taxes. So instead of NIAT, the bottom-line amount reported is the total by which revenues exceed expenses. Ratio Analysis A ratio analysis combines information made available by the finance and accounting depart-
- 12. ments to help managers evaluate various operations in the organization. Healthcare managers are usually interested in four categories of ratios: • Liquidity ratio: Measures the organization’s ability to pay its short-term obligations on time • Activity ratio: Measures efficiencies in organizational operations • Leverage ratio: Measures organizational debt and risk • Profitability ratio: Measures organizational profits Although other ratios may be calculated, these four categories offer healthcare managers a quick look at an organization’s financial well-being. Managers should avoid the tendency to overem- phasize any single ratio; instead, they should look at the group of ratios together. Managers can compare ratios from the current year with those from previous years or with averages in the industry to gain further understanding of the organization’s financial standing (Reilly, Minnick, & Baack, 2011). Figure 6.2 Elements of an income summary f06.02_HCA340.ai Sales (Revenues) –Cost of goods sold Gross profit –Operating expenses Gross operating income
- 13. –Depreciation Net operating income –Other unusual expenses +Other unusual income Net income before taxes –Taxes Net Income After Taxes (NIAT) Patient payments Insurance payments Governmental reimbursements $12,000,000 15,000,000 25,000,000 42,000,000 <12,000,000> 30,000,000 <18,000,000> 12,000,000
- 14. <5,000,000> 7,000,000 <1,000,000> +3,000,000 9,000,000 <1,800,000> $7,200,000 Financial Governance and Working Capital Policy Chapter 6 Working Capital Policy Financial managers in both nonprofit and profit-seeking entities have the duty of overseeing an organization’s cash flow. This includes making sure the organization maintains sufficient funds to operate on a day-to-day basis through oversight of current assets and current liabilities. Working capital is a comparison of the amount of current assets an organization has on hand in relation to its current liabilities. Using the information from a balance sheet, a financial manager can compute the organization’s amount of working capital as follows: Working capital = Current assets – Current liabilities
- 15. Working capital can be generated in many ways, including through selling new or additional shares of stock, selling long-term bonds, or securing other types of loans in order to generate the funds needed to ensure that the organization remains liquid. In many healthcare organizations, management of working capital creates some difficulties, which often emerge as a result of timing. For example, someone who receives medical care may be charged the copayment amount during the actual hospital visit; however, that copay is only a small part of the balance due for anything more complicated than a routine examine. Often, a considerable amount of time passes before the organization receives any government or insur- ance company payment. Only then is the patient billed for the remaining balance so that payment can be rendered. As noted earlier, Medicare and Medicaid can be notoriously slow at rendering payments. While waiting for this payment, the organization must pay bills for medical supplies, payroll expenses, and other costs, all of which are due nearly immediately. Thus, working capital requires extra attention by financial managers (McLean, 1997). Effective management of working capital creates a series of benefits. First, an effective working capital policy means the healthcare provider will remain liquid, which in turn means that the organization will always have funds available to meet obligations such as payroll and tax pay- ments. Second, organizations that routinely pay bills on time generate goodwill with suppliers, manufacturers, and other vendors. The net outcome of this goodwill can be that the hospital
- 16. will receive the most attentive care from those vendors. Third, an effective working capital policy establishes a line of credit over time, so that the organization can borrow money in case of finan- cial emergencies. Bundled Reimbursements: A Potential New Working Capital Challenge In the past, when a person with an acute medical problem arrived at the hospital, the individual received the necessary care and was then made ready for discharge. If the patient required additional services, such as rehabilitation, a home health facility, or a skilled nursing facility, each treating unit (that is, the hospital and every other organization the patient visits) billed the person and the gov- ernment (such as Medicare) separately for each service, or “silo” of care. Under a system proposed in the U.S. legislature as an addendum to the Affordable Care Act, the government (Medicare) would pay one provider—typically the hospital—for the entire patient episode, from entry into the system to a return to health. The entity or hospital would then divide the reimbursement among all orga- nizations that served the patient. (This addendum has not yet been passed or enacted.) The reasoning behind the bundled payment system is to increase efficiencies in care. Under this plan, patients would no longer receive multiple billings, and the government would only make a single payment—all with the goal of reducing redundancy in postoperative-care facilities (Jackson, Greis, & Rawlings, 2009).
- 17. Long-Term Financial Governance Chapter 6 However, hospital administrators have raised major concerns about how such a system would be administered. Under the plan, each hospital would be placed in a decision-making role regarding the amount each connected unit should receive for a patient’s care. Many healthcare administra- tors have expressed concerns about conflicts with other organizations, lowered levels of reim- bursement, and the confusion created by the paperwork of such a system. This new proposal has elicited two suggested responses. The first is a vertical integration system, in which the hospital would purchase or establish the linking levels of care under its ownership, thereby keeping all payments within one billing entity. An example of a vertical integration sys- tem is a hospital that purchases a rehabilitation facility and an extended-care organization. A patient who becomes incapacitated would first stay in the hospital, would then use the services of the rehab center, and might finally be placed in an extended- care setting. When the person is finally discharged, the hospital would bill that patient for all activities at once. The hospital would then distribute monies received to each aspect of its operations. The second response involves the development of network embeddedness systems, in which informal networks of organizations would divide reimbursements on a routine basis (Dacin, Ventresca, & Beal; 1999). An example of an embedded network is an informal combination of
- 18. healthcare organizations under separate ownership in which each receives reimbursements and then the payments are distributed among the members. In the bundled payment approach, the organization that receives the payment often faces a chal- lenge in deciding on the amount to be allocated to the other units involved in the patient’s care. One way to solve this problem is to devise a transactions cost approach, in which each activity is assigned a cost to be reimbursed as a percentage of the total payment to the primary provider. The percentage should take into account the costs and the allowable reimbursements for each unit that treated or cared for the patient. Another continuing challenge with the bundled payment approach involves working capital issues. Each unit incurs expenses associated with the patient’s care that are entitled to reim- bursement. Unfortunately, a substantial amount of time might pass before any payment is sent by the primary organization (that is, the organization that received the full bundled payment) to the individual unit. Furthermore, disputes among managers from individual units may arise regarding exactly how much each unit should be granted as a percentage of the patient’s total care package. Estimating and keeping on hand the amount required to maintain cash flow and make payments under such a system adds an additional complication to a system that already experi- ences significant problems (Shay, 2013). 6.2 Long-Term Financial Governance In addition to working capital policy, another major
- 19. responsibility held by financial managers in both nonprofit and profit-seeking ventures involves ensuring that the organization tries to achieve consistent outcomes across all time horizons. This process requires the manager to mesh short- term operational duties with long term strategy making. In the areas of finance and accounting, managers work to integrate activities by obtaining funds for and managing the organization’s monetary well-being so that the organization’s top management team can create effective strate- gies that lead to future success. In the long term, two major concerns of financial managers are dealing with pricing issues and creating long-term financial instruments. Long-Term Financial Governance Chapter 6 Pricing Pricing includes institutional marketing and financial considerations. In some instances, govern- ment programs determine the prices charged for medical systems. For example, the Medicare prospective payment system (PPS) method of reimbursement establishes prices and payments based on predetermined, fixed amounts. Payments for individual services are based on the PPS classification system for each service. The Centers for Medicare and Medicaid provides separate prospective payment systems for individual diagnostic related groups (DRGs), such as acute inpa- tient hospitals, home health agencies, hospice, hospital outpatient, inpatient psychiatric facilities,
- 20. inpatient rehabilitation facilities, long-term care hospitals, and skilled nursing facilities (Centers for Medicare and Medicaid Services, 2013c). In marketing, methods for setting prices may be based on costs, profit goals, supply and demand, or competition. Each approach assists the finance team in pricing healthcare products and services. Costs When calculating price based on cost, the first determination involves the difference between fixed costs and variable costs (Higgins, 2011). Fixed costs are expenses incurred that are not affected by the volume of sales; the provision of healthcare services; or revenues from the patient, the insurance company, and the government. Examples of fixed costs include building payments (fixed loan or lease payments), annual salaries, and utility bills. An important component of fixed costs involves deciding how much to allocate to each service. For example, if a physician’s prac- tice spent $200,000 per year on fixed costs, and the physician had 8,000 appointments per year, then the fixed cost per appointment would be $25 per appointment ($200,000 ÷ 8,000). If the physician were able to increase the number of appointments to 10,000 per year, the fixed cost per appointment would drop to $20 per year ($200,000 ÷ 10,000). Fixed-cost allocation applies to hospitals, physician clinics, and any provider of medical supplies or equipment. Variable costs are directly related to volume or revenues. In healthcare, variable costs include
- 21. billings for physician services; diagnostic procedures, such as reading an X-ray or conducting a blood test; medical supplies, including materials for bandages and stitches; and other per-patient or per-visit expenses. A greater number of patients incurs a higher total variable cost, although regardless of the number of patients, the variable cost per patient remains relatively stable. Only when a hospital pays extra expenses—such as overtime wages to nurses and support staff mem- bers in the case of a major emergency like an accident that injures a great number of people— would variable costs per patient rise. Total costs are calculated by adding total fixed costs to total variable costs. Total cost per patient results from adding fixed costs per patient to variable costs per patient. These figures may then be used to set prices based on costs. Two forms of cost-based pricing are markup pricing and cost-plus pricing. A markup pricing approach assigns a percentage to be added to the total cost per item. Assume, for example, that the total cost per patient visit is $40 ($25 fixed costs + $15 variable costs). The practice believes that a 50% markup represents a reasonable amount. Therefore, the patient would be charged $60 for the office visit ($40 × 0.5 = $20; $40 + $20 = $60). Another option is to assign markup to total costs rather than to costs per visit. Suppose a walk-in clinic’s total fixed costs amount to $500,000 per year, and its total variable costs are $100,000 per year. Its total costs would be $600,000 per year. If the
- 22. organization used the same 50% markup, Long-Term Financial Governance Chapter 6 then it would add $300,000 ($600,000 × 0.5) to total charges, resulting in a total amount of $900,000. The $900,000 would then be divided by total patient visits. If 100,000 patients visited the clinic during the year, each would be charged $90 per visit ($900,000 ÷ 100,000). Such an approach is unlikely, however, due to the wide variance in variable costs per visit and per patient. For example, an infection would incur one set of variable costs, whereas setting a leg fracture, complete with X-rays and other services, would lead to much higher variable costs. The main advantage of markup pricing is precision in pricing for each action. The disadvantage is the extra time involved in making calculations for each individual item or service. Cost-plus pricing adds a fixed amount to the total cost per patient. Suppose the total cost per patient visit is $40. The unit decides to charge each patient an additional $25 per visit. Thus, the charge for the visit would be $65 ($40 + $25). Cost-plus pricing based on total costs adds a fixed amount to total costs. If total costs equal $600,000 for the year, and the organization charges a total of $400,000, then total charges would be $1,000,000. For 100,000 patients, the visit charge would become $100 ($1,000,000 ÷ 100,000).
- 23. The primary advantage of cost-plus pricing is the ease of calculation. The disadvantage is that some patients might feel overcharged, while others are undercharged. For example, one patient visit may take a physician 30 minutes or more to resolve, while another only takes 5 minutes, yet the two patients are charged the same amount. To some, this might seem unfair, even though the real charge is for a doctor’s expertise more than for his or her time. Costs and Healthcare Pricing Each type of healthcare provider can use costs to develop charges (or the “price” of a service). The form of pricing is adapted to the type of healthcare being pro- vided. For example, dentists, physicians, psychiatrists, and others might use markup or cost-plus pricing to establish rates for office visits. Then, they might examine individual services to set charges using one of the two methods. The charge could be based on the level of expertise and precision required, combined with a charge for less-direct costs, or an activity-based costing system (Canby, 1995). For example, a dental procedure, such as a root canal, would carry a higher price than a typical dental visit due to the expertise required to perform the procedure. In addition, the procedure requires specialized equipment, the cost of which would be partially allocated to the procedure. In this case, variable costs include a charge for the assistance of a dental technician, as well as the costs of a numbing injection, gauze or cot- ton, and other items. When determining activity-based costs, financial officers bear in mind that an established price
- 24. or charge will be subject to a variety of forces, including the following: • Provider discounts • Provider write-offs © Stockbyte/Thinkstock ▲▲ Medical services, such as computed tomography (CT) scans, can be priced using markup or cost-plus methods. Long-Term Financial Governance Chapter 6 • Third-party payment agreements • Patient copays and coinsurance • Low- versus high-payer source • Fairness concerns • Payer mix and cost shifting These items affect the actual revenue stream that the organization receives. Payer source con- stitutes a primary concern for many healthcare providers: A low-payer source is an entity that makes payment for a medical treatment, yet the amount is less than remuneration paid by other entities. Three examples of low-payer source funding include Medicare, Medicaid, and many managed-care plans. High-payer source organizations include some insurance policies and ben- efits from workman’s compensation plans. Some evidence suggests that low-payer source patients make fewer visits to healthcare facilities and, upon discharge from treatment, are often less func-
- 25. tional, meaning they have not had a complete recovery or are still not healthy (Nof, Rone-Adams, & Hart, 2007). With regard to fairness concerns, the American Medical Association (AMA) advocates accurate valuations of all physician services. The AMA designed the resource-based relative value scale (RBRVS) to ensure that every physician service and specialty is represented with regard to pay- ment policies and systems. The RBRVS figures are based on evaluations and recommendations of the AMA and its Specialty Society Relative Value Scale Update Committee and include any new or revised services. The committee undertakes broad reviews of the RBRVS every five years (AMA, n.d.-c). In addition, the Centers for Medicare and Medicaid (2013a) provide the Healthcare Common Procedure Coding System (HCPCS), a numeric coding system maintained by the AMA. The uniform coding system “consists of descriptive terms and identifying codes that are used pri- marily to identify medical services and procedures furnished by physicians and other healthcare professionals. These healthcare professionals use the system to identify services and procedures for which they bill public or private health insurance programs.” The objectives of the system are uniformity and fairness. A payer mix refers to the amounts provided as payments by various providers, including govern- ment sources and insurance. The mix determines total revenues that the healthcare organiza-
- 26. tion receives. Cost shifting, which is the practice of charging private payers, such as insurance companies, more in response to shortfalls in public payments, has long been part of the debate over healthcare policy. Although some evidence suggests that the amounts of such shifts are not dramatic, the subject remains controversial (Frakt, 2011). An organization such as a pharmaceutical company might use a form of pricing that is entirely different from the activity-based approach. The development of individual drugs often takes years of research and testing, followed by government approval (by the Food and Drug Administration). Only then can the drug be released to the general public. In addition to these costs, advertis- ing and personal selling costs also accrue. The pharmaceutical company’s management team remains acutely aware that a window of 12 years is in place for the organization to charge as much as is needed to recover startup costs (12 years is the length of a medical patent). After that win- dow, other companies can manufacture generic versions of the drug and offer them at much lower prices. Thus, managers try to set prices that capture all startup costs, plus a reasonable return on investment in that 12-year period. This explains why new drugs to the market are often quite expensive for patients and hospitals. Long-Term Financial Governance Chapter 6 In summary, the management team, working in conjunction with the finance and accounting
- 27. departments, can set charges or prices using fixed and variable costs as the starting point. Each situation remains unique, however, and the pricing approach is adjusted according to the type of provider and the types of services being rendered. Pricing Based on Profit Goals Healthcare providers that seek to make profits, including pharmaceutical companies, medical equipment manufacturers, medical supply providers, some hospitals, and private practitioners, can incorporate cost information with desired profit targets, or the amount of revenue they intend to generate from a given product or service. Some hospital managers may not use the term profits; instead they refer to the degree to which revenues exceed expenses. In either case, a common method for analyzing profitability is a break-even analysis, which identifies the point at which the total costs incurred are equal to the revenue received. Figure 6.3 provides a visual portrayal of the relationships among fixed costs, variable costs, volume, and profits. A break-even analysis can be calculated for individual services and is valuable when making deci- sions about how much to charge for the use of a major piece of medical equipment, such as a mag- netic resonance imaging machine. Break-even points can also be calculated based on the volume of revenues, which best fits a provider that offers a variety of services. A break-even analysis also has use for nonprofit settings, as managers can use the information to set charges high enough to create funds for altruistic purposes or for the expansion of
- 28. medical services offered rather than profit goals (Van Horne, 1974). Figure 6.3 Break-even analysis f06.03_HCA340 D Volume B C A Cost Loss Profit Key Revenues Break-even point Total cost Variable costs Fixed costs Long-Term Financial Governance Chapter 6 Competition-Based Pricing
- 29. In some instances, pricing based on the competition is most appropriate for healthcare orga- nizations. For example, many over-the-counter medicines compete with generic drugs. Insurance companies establish premium rates based, in part, on what other competitors charge. Psychologists, psychiatrists, dentists, and other providers are often aware of the fee schedules of others in a geographic region. However, as has been stated earlier, the complicating factor for most healthcare service providers is that the actual price may be extremely difficult to identify. Individuals with health insurance policies who seek care pay an amount that is vastly different from the fee or price of a service that appears on the indi- vidual’s bill or statement. As a result, setting prices based on competition becomes problematic. Three competition-based pricing strategies include above the competition, meet the competition, and below the competi- tion. Highly exclusive plastic surgeons may routinely price services above those charged by others, whereas eyeglass and hearing aid providers often use competition-based pricing. Some organizations advertise their prices to make it well- known to the public that the products are being sold at the lowest price in the area. In most other situations, however, a healthcare provider does not want to be known as pricing services on the cheap, because price does imply quality. Supply and Demand Pricing Although pricing based on supply and demand is common in many private-sector industries, it only applies to a rare num- ber of circumstances in healthcare. Most of the time, revenues
- 30. and costs provide better-quality information for healthcare financial officers. Supply-and-demand factors affect prices in circumstances in which only a small number of individuals have a disease or medical condition, as a low demand for any remedy, such as a medicine, may severely drive up the price. Additional Considerations The unique status of healthcare in the community creates additional constraints on financial officers. Additional factors that influence pricing programs include the following: • State and federal laws and regulations • Antitrust and fair pricing laws • Joint Commission recommendations Government regulations may influence the amount that a provider can charge. Various laws that create antitrust provisions and fair pricing standards have been put into place to ensure that healthcare providers do not create monopolies capable of charging prices without constraints. In addition, the Joint Commission helps set standards for various healthcare services as part of its accreditation program (Joint Commission, 2013). © Digital Vision/Thinkstock ▲▲ Some forms of medical care, such as eyeglass prescriptions, are priced based on competition. Long-Term Financial Governance Chapter 6
- 31. W E B F I E L D T R I P Healthcare Blue Book provides a service that is intended to help consumers determine fair prices for healthcare services and to make comparisons between prices in their area versus prices in other areas. Visit http://www.healthcarebluebook.com, enter your zip code, and search for the prices of a few procedures and services. Then search the same procedures and services in the area code of a city or town that is very different from your own, whether in size or geography. • Is there a difference in price for the procedures and services in your area versus those in other cit- ies? What do you think might account for any differences? Providing Financial Resources Another primary function provided by the chief financial officer involves the selection and imple- mentation of the long-term financial instruments used to provide for major capital expenses. Such expenses include the purchase of a new building, expansion of a current facility, the pur- chase of expensive major medical equipment, and the acquisition of any other large asset that will be used over a period of years. The four primary long-term financial instruments, or legal documents representing monetary value, are bonds, loans, stocks, and leases. Bonds Bonds are fixed-payment instruments that are issued and sold in order to raise capital. A bond instrument’s terms include the amount of the bond (money paid
- 32. to purchase it), a specified interest rate, and the terms of repayment. Some bonds are bought and sold by various financial organizations. Buyers may find them more or less lucrative depending on changes in prevailing interest rates and the buyer’s trust in the bond issuer. The first distinction in bond instruments depends on the nature of the organization issuing them. A for-profit bond’s interest payments provide taxable income to bondholders. In contrast, a bond issued by a nonprofit healthcare organization may offer tax-free revenue or interest income to those who purchase the bonds. Bonds normally require funds to be set aside so that they are repaid at a specified time. The bond’s sinking fund represents these monies on the company’s balance sheet. Coupon bonds require regular interest payments (monthly, quarterly, annually) to bondholders. Other bonds allow for repayment of both the principal and the interest when the bond is redeemed. The primary benefit of a bond to a for-profit hospital or skilled nursing facility is that the interest paid on the instrument can be listed as an expense on an income summary, which reduces the real interest rate for the funds. For example, a bond that pays 5% would cost the organization 1 minus the tax rate times the interest level. Thus, if the corporation paid a 20% tax rate on income, then the effective rate for the bond would drop to 4% ([1 – 0.2] × 0.05 = 0.04). The primary disadvantage of a bond, to both for-profit and
- 33. nonprofit organizations, is that pay- ments to sinking funds must be set aside and cannot be used for other purposes. This limits the organization’s financial flexibility to some extent. Furthermore, failure to make interest payments or to redeem bonds places the organization in default, which means bonds imply at least some http://www.healthcarebluebook.com Long-Term Financial Governance Chapter 6 level of risk. Bond-rating organizations specify the degree of that risk. The lower the rating, the greater the level of risk. Investors expect a risk premium, or a higher level of interest, for bonds with lower ratings (Marlowe & Matkin, 2013). Loans Financial institutions (e.g., banks, savings and loans) and other lenders make loans to individual organizations. Loans are less structured than bonds, with more flexible terms. Hospitals acquire loans to cover shortfalls in working capital and other financing needs. Many features of loans are the same as those for bonds, with the amount, duration, and interest rate spelled out in a loan contract between the healthcare and financial organizations. Healthcare organizations offer collateral to ensure loan repayments. A hospital with a debt-free building could use that facility as collateral to secure a loan for some other purpose, such as the acquisition of a cutting-edge piece of medical equipment. This feature of loans provides the
- 34. healthcare financial officer with additional flexibility. Loan interest is tax deductible for profit-seeking organizations. Each loan carries with it a level of risk, however, due to the possibility of default. Stock A relative minority of healthcare organizations issues stock. The issuance of stock allows the organization to collect funds for long-term projects. In exchange, shareholders expect to receive dividends, or earnings distributions, which are not tax deductible for the organization that issues the stock. Dividends are paid out of an organization’s after-tax profits. In addition, shareholders expect a risk premium, which further increases the cost to the healthcare facility. The primary benefit of stock is that it is issued in perpetuity, which means no sinking fund or repayment is required. Not-for-profit healthcare organizations cannot issue stock. Leases Any number of healthcare organizations can benefit from leasing arrangements. A leasing arrangement can help an organization obtain not only major medical equipment but also office equipment, such as copiers and computers. In some instances, leases may apply to build- ings that house medical services. Lease terms specify an amount to be paid, the length of the lease, and any special arrangements, such as maintenance and repair.
- 35. The advantages of leasing include the ability to continually upgrade the technology in use. As the lease for one piece of equipment expires, a newer version of the equipment can be acquired with a new lease. Lease payments are tax-deductible expenses, thereby reducing the net cost. Many organizations also benefit from maintenance program offered by providers of leased equipment. The primary disadvantages of leasing include a fixed obligation that is similar to a sinking fund—normally, lease payments are made monthly. In addition, the organization becomes locked in until the lease expires. Thus, an obsolete or unreliable piece of equipment must be kept until that point. © iStockphoto/Thinkstock ▲▲ Fleets of ambulances can be acquired using leasing arrangements. Long-Term Financial Governance Chapter 6 Donations One unique form of fund raising that appears in the healthcare environment is donations. Donors
- 36. provide funding for parts of a hospital (e.g., a wing or a medical practice) and other larger pur- chases, often in exchange for naming rights or for having the donor’s name prominently displayed in some way. Fund-raising programs can be used to finance shortfalls in year-to-year operations, as well as larger projects and tangible organizational features. The benefits of donations include increased visibility in the community for both the donor and the healthcare provider. Some funds can be set aside in savings and investment programs. The pro- ceeds can then accumulate until a major purchase can be made or the proceeds can be invested into the organization’s general fund. The costs associated with donations are those incurred in fund-raising programs, often including the salary of the person in charge. It is important to note the dramatic impact donations have on the healthcare community, including many local and charitable hospitals. C A S E The Skin Rejuvenation Center Dr. Richard Jorgenson opened his dermatology practice nearly a decade ago. Early in the process, he advertised extensively in the local newspaper, on the radio, and in a regional magazine. Over time, physician and former patient referrals helped his practice grow to the point at which he was able to retain two skilled nurses and an office staff consisting of three additional individuals. In the past year, a new opportunity arose: Dr. June Lee, a
- 37. recently graduated dermatologist, opened a practice on the other side of the city. Focusing on female patients and children with skin prob- lems, her practice was growing steadily. Dr. Lee approached Dr. Jorgenson with a proposal: The two could combine to open The Skin Rejuvenation Center in the middle of town. The center would provide beautification services related to dermatology, such as dermal abrasion, chemical peels, Botox injections, and laser resurfacing. These treatments would help those with aging-based problems, such as wrinkles, age spots, sun damage, and skin problems resulting from smoking. To supplement these programs, the center would also provide other services, such as facials, body scrubs, body masks, and body wraps. The organization would also sell skin products, including moisturizers, acne medicines, and various oils and waxes. The Skin Rejuvenation Center would also sell safer tanning products that do not require sun exposure. A third element of the operation would involve minor surgeries, including permanent makeup; hair removal; and treatments for warts, moles, and beauty marks. This would make the center a nearly full-service beautification operation. Dr. Lee noted that some of the services would qualify for insurance benefits, while others would not. She also pointed out that some of the services would receive payments as they were rendered. Dr. Jorgenson wondered whether the company would primarily benefit Dr. Lee’s patients, or if oth- ers would be inclined to visit the center.
- 38. After consideration by both sides, The Skin Rejuvenation Center opened. The two physicians located a building in which they could create a lease-purchase contract. They needed to renovate (continued) Accounting in Healthcare Chapter 6 6.3 Accounting in Healthcare Healthcare administrators consider both short-term and long- term financial decisions care- fully. Part of this process includes planning annual budgets, overseeing cash flows, and working to ensure that costs remain at acceptable levels. Both nonprofit and profit-seeking organiza- tions maintain accounting records and conduct other activities that support the organization’s operational, tactical, and strategic intent. This section examines accounting practices related to budgeting, accounts receivable management, accounts payable management, cost controls, and auditing of operations. Budgeting Budgeting represents the area in which financial and accounting activities overlap the most. In addition, managers from other departments, including human resources and those who oversee clinical, administrative, and support staffs, are often involved in the process. Each manager seeks sufficient funding to effectively operate his or her individual
- 39. department. As a group, these indi- viduals identify the needs of the organization, as well as the costs of those items, both for annual operations and the long term. In larger healthcare organizations, two types of budgets require attention: the capital budget and the operating budget. Capital Budget A capital budget assists in planning for major expenditures and acquiring the funds needed to finalize such purchases and lease arrangements. Capital budgeting programs incorporate mana- gerial plans with accounting and financing arrangements (Gapenski, 2009). Healthcare manag- ers, working in conjunction with other leaders, identify the major (fixed) assets to acquire, such as a building, a renovation, a fleet of ambulances, or other medical equipment. The capital budgeting process involves the following steps: 1. Identify the required asset(s) and the funding needed to purchase them. 2. Estimate the useful life of the asset(s). 3. Determine the method of depreciation that applies to the asset. 4. Specify the nature of payments to be made. The required resources are based on the price of the asset(s) to be obtained. Managers make deci- sions about how to procure the assets, whether through bonds, loans, stock issues, or leases. The the interior to meet the medical and aesthetic requirements for this type of business. The two der- matologists knew they had entered a new and exciting period in their careers.
- 40. In answering the following questions, it may be helpful to review Sections 6.1, 6.2, and 6.3. 1. How would the combination of business services and products assist in the area of working capital? 2. What method of pricing should apply to each of the three types of services The Skin Rejuvenation Center plans to offer? 3. Beyond the lease for the building, what type of financing should the two physicians use to acquire the necessary equipment and furnishings? What advantage would there be to the lease? To the other forms of financing? 4. Identify the fixed and variable, direct and indirect costs associated with this new company. Accounting in Healthcare Chapter 6 goal is to maintain a reasonable cost of capital that balances costs with risks, fixed obligations, and other considerations, such as donations. The asset’s useful life should be estimated and established between the healthcare organization and the vendor selling the asset. The length of the life determines in part how the item will be depreciated and the method of payment to be made. The method of depreciation varies according to the following:
- 41. asset’s years of useful life, whether an asset retains or quickly loses value after its purchase, the organization’s tax situation, and managerial preference. Accelerated depreciation methods are employed for assets that quickly lose value or by organizations seeking to reduce immediate tax liabilities by front-loading the expensing of items. Organizations employ straight-line depreciation when the useful life delivers a consistent value over its life span. Accelerated depreciation applies to circumstances in which an asset quickly loses value or when doing so improves an organization’s tax situation for the early years of the asset’s life (Oliver & Horngren, 2010). The nature of payments results from the type of financial instrument. A bond requires a sinking fund. A loan and a lease will feature monthly, quarterly, semiannual, or annual fixed obligations. Stocks include a dividend policy stating how and when dividends will be paid to shareholders. All of these payments are built into the operating budget prepared by the accounting office for each year. An additional major capital expenditure that has become increasingly common in the healthcare system occurs when a major facility, such as a hospital, purchases the practice of an independent physician, thereby bringing that practice under its operating umbrella. Capital must be raised to make such purchases. Operating Budget and Revenues An operating budget maps expected revenues and then allocates the funds to individual depart-
- 42. ments and activities for their expenses, normally over a one- year period. The annual document specifies the nature of all revenues to be received. Revenues accrue from third-party reimburse- ments and patient payments. Third-party reimbursements take various forms, including those itemized in Table 6.1. Table 6.1 Forms of third-party reimbursement Form Explanation Example Fee for services Full charge for a service Annual exam Per diem Dollar amount per day for care Hospital room charge Nursing facility daily charge Per diagnosis Amount charged for a diagnostic service Read an X-ray Bundles Fixed amount shared by providers Set of doctors, one patient Capitation Fixed amount per enrollee per month for specified services Managed-care organization charge per patient Government Reimbursement Medicare
- 43. Medicaid Accounting in Healthcare Chapter 6 Accounts receivable includes amounts due for all services that have been rendered or items that have been sold for which payment has not yet been made. Accounts receivable management constitutes a critical activity in the accounting department of most healthcare organizations (Sachdeva & Gitman, 1981). Receivables are collected from third-party reimbursement organi- zations, from government organizations, and then from patients. A fully developed accounts receivable program incorporates the activities detailed in Table 6.2. Table 6.2 Elements of accounts receivable management Element Explanation Precertification Prior to admission; verifies the patient has insurance Medical records Coding of all evaluations, treatments, medicines, and other medical services Billing Itemized statements sent to patients, insurance providers, and government agencies Collection Receipt and deposit of funds sent; financial counseling to patients
- 44. (including setting up payment programs) Accounting entries Recording of all payments and nonpayments for accounting purposes Legal Oversight of contracts, litigation policies, federal regulations, and patient rights Compliance Detection and reporting of fraud and abuse Operating Budgets and Expenses After the accounting office establishes the total amount of expected revenues for the upcom- ing year, operating budgets for individual departments and activities can be established. Three potential forms of allocation can be made for these units: across-the-board, relative-amount, and variable or flexible budgets. An across-the-board operating budget estimates the growth, stability, or decline of revenues expected in the coming year. Each department then receives a budget allocation that mirrors the change in revenues. For example, if a hospital board expects a 3% increase in revenues, then each department would receive a 3% increase in its annual operating budget. The same type of adjustment would be made for budget decreases or for a flat budget. Across-the-board budgets are common in government organizations, including Medicare and Medicaid. A relative-amount operating budget allocates funds to various departments based on need. To determine need, financial management often conducts a cost–
- 45. benefit analysis, which involves adding the benefits of a business-related program or action and then subtracting the costs asso- ciated with that program or action. If, for example, a cost– benefit analysis determined that a laboratory had been underfunded, and services to patients and physicians had suffered as a result, then additional resources would be allocated to that unit, and other units would receive lower allocations. A variable or flexible operating budget adjusts departmental allocations during the course of the year. If higher-than-expected revenues occur, then budgets are adjusted upward. If revenues decline, the budgets reflect that change as well. Both across- the-board and relative-amount bud- gets can be adjusted using the variable approach. Accounting in Healthcare Chapter 6 Healthcare managers in various departments become quickly familiar with how budget alloca- tions for expenses are made. Each year they make budget requests that often include requests for extraordinary expenditures. It becomes the role of top management to make judgments about which applications are most viable. Cost Allocations and Cost Control Healthcare accountants hold two major responsibilities in the area of costs. First, they are charged with allocating costs in as precise a manner as possible for each form of healthcare. Second, they
- 46. assist in trying to reduce or manage the costs of various materials and activities. The previous section described concepts regarding fixed and variable costs and pricing meth- ods based on those costs. In addition to those costs, accountants provide information regarding direct and indirect costs. Direct costs in healthcare are those that can be attributed to a specific treatment format for a patient or activity. Direct costs include physician fees, medical supplies, medical equipment, nursing care, and any other item directly associated with helping a patient. Indirect costs in healthcare constitute those that cannot be attributed to a specific patient or form of service, such as most support staff activities, including patient safety, food ser- vice, and janitorial services. Calculations of direct and indirect costs compile impor- tant information for billing practices and third-party payment requests that are sent to insurers and governmental agencies. To help control costs, accounting manag- ers compute important numbers regard- ing inventories, payroll figures, and other expenses, such as supplies for bathrooms for visitors. Inventory control constitutes a key activity provided by the accounting department. The management of medical supplies balances two key factors: main- taining sufficient inventory and not carry- ing excess inventory. Sufficient inventory is needed so that the organization does not experience a stock out, or the failure to have a crucial medicine or medical supply on hand. A
- 47. stock out can lead to a negative outcome for a patient. Excess inventory, on the other hand, leads to expensive carrying charges, or the costs associated with nonuse of an item and the finance charges related to that excess inventory. The activity-based costing system mentioned in Section 6.2 creates a valuable method of inven- tory control. For example, the ABC inventory control method places drugs into three categories. The A group holds highly expensive drugs that must be carefully monitored so as to not engender high carrying charges. The B group has moderate-cost medicines that require scrutiny but to a lesser degree than the A group. The C group represents items that remain important for day-to- day activities but that have low costs (Nowicki, 2004). A major element in cost control involves uncompensated healthcare, in which uninsured indi- viduals receive medical treatment but cannot pay for it or in which individuals fail to pay their portion of the expense, such as coinsurance. Financial officers must decide how to allocate these costs to the organization. Many nonprofit healthcare institutional leaders consider care to those © Huntstock/Thinkstock ▲▲ Direct costs are those attributed to a specific treatment or activity. Accounting in Healthcare Chapter 6
- 48. who cannot afford it to be a primary altruistic mission of the organization. In profit-seeking set- tings, however, decisions regarding who receives care are, in part, dictated by the government. For example, emergency rooms are mandated to treat anyone needing emergency care, regardless their ability to pay (Hadley & Holahan, 2004). Auditing Healthcare organizations engage in two forms of auditing: internal and external. An internal audit seeks to ensure that accounting and financial operations and statements are accurate and that the systems in place protect against intentional or unintentional malfeasance. Internal audits may be conducted either by an accountant specifically retained by the organization to provide such services or by an outside provider that has been retained by the organization. For example, the Catholic Healthcare Audit Network provides internal audits for numerous Catholic health- care organizations and facilities. External audits are imposed by an outside force, such as for a government requirement. Any healthcare organization that participates in Medicare becomes subject to an annual external audit. Many financial organizations require external audits before an organization can receive a loan or assistance in the sale of bonds or common stock. For both internal and external audits, typical inspections are made in the following areas: • Accuracy of financial records • Accuracy of human resource records, including time cards, sick leave pay, and accruals
- 49. of benefits • Management of physical assets, including maintenance • Management of purchasing procedures • Analysis of uncompensated care • Protection against financial conflicts of interest by various parties • Protection against fraud perpetrated against outside organizations (e.g., against the govern- ment or insurance companies) • Protection against fraud perpetrated against the healthcare organization • Protection against inurement, or gaining a financial advantage through insider status Audit reports tend to be sweeping documents covering these areas. Auditors point out problems and make recommendations regarding potential solutions. It is then up to the organization’s financial, accounting, and corporate executives to make sure that problems and deficiencies are corrected. Cases of illegal activities must be reported to the appropriate government agency. Chapter Summary Chapter 6 Chapter Summary Financial governance in the field of healthcare involves oversight of day-to-day operations that require financing and planning for and implementation of instruments that provide for the orga- nization’s long-term financial needs. Healthcare managers employ balance sheets to understand
- 50. the organization’s basic standing with regard to assets and liabilities. They use the income sum- mary to determine whether revenues exceed expenses. And they use ratios to evaluate other monetary circumstances of the organization. Working capital policy oversees the organization’s cash flow, ensuring that sufficient funds are available to pay bills as they come due. Healthcare managers understand that cash inflows often lag outflows; as such, they take the necessary steps to make sure the organization remains solvent. C A S E Accounting for Altruism John Mulvaney faced a unique challenge. As the chief financial officer (CFO) for Merciful Hospital, he had been given the directive to make certain the organization stayed true to its name. The board of directors had established a policy that 10% of the hospital’s excess of revenues over expenses (in essence, the “profits” for this nonprofit organization) would be directed to granting care to those without insurance, those with low incomes, and others in difficult financial circumstances. On the surface, the mandate seemed fairly straightforward; however, several issues quickly emerged. First, if the policy were widely publicized in the community, would some patients believe they were being charged extra so that others could receive free medical care? This might lead some to seek treatment elsewhere. How might that decision affect revenues?
- 51. Second, the hospital had to accept many payments as dictated by government forces. Medicare, Medicaid, and other payers have established set amounts for various treatments, and these orga- nizations are often categorized as low payers. How would it be possible to create circumstances in which costs would be sufficiently low so that revenues would exceed expenses for those services? Third, the most lucrative procedures (in terms of revenues versus costs) are those that are not nor- mally covered by insurance, such as elective surgeries for cosmetic appearance. How should these be priced relative to other treatments? John also considered other sources of revenues not directly related to patient care. He believed it would be wise to establish a foundation with the sole purpose of funding altruistic care. His dilemma was how to account for monies received with regard to an income summary. John hoped that donations would be placed into an ongoing fund, with only the interest received being used to support the altruistic program. In the end, John was pleased by his organization’s desire to take care of the most vulnerable. His task was to figure out how to account for and finance the intention. 1. How should free or reduced-price services be calculated on accounting forms? Which portion would be revenue? Which portion would be cost? 2. How might these altruistic programs affect the organization’s
- 52. working capital? 3. How would the organization account for direct and indirect costs for services provided free of charge? 4. What sources of financing, beyond donations, might be useful for the altruistic care program? Key Terms Chapter 6 Healthcare pricing is typically based on costs, profits, or the competition. Managers evaluate fixed and variable costs and assign them to individual services, thereby establishing a base price, or charge. In some settings, prices are set to match, exceed, or undercut the competition. Rarely do supply-and-demand forces affect charges in healthcare settings. When acquiring large assets, healthcare financial officers consider the use of bonds, loans, com- mon stocks, and leasing. Each option creates differing costs, risks, and cash flow issues. Accounting practices in healthcare include budgeting, accounts receivable management, accounts payable management, cost controls, and auditing of operations. Capital budget and operating budgets represent the two main forms of accounting practices. The capital budget assists in plan- ning for major expenditures and acquiring the funds needed to finalize such purchases and lease arrangements. An operating budget maps expected revenues and then allocates the funds to
- 53. individual departments and activities for their expenses. Healthcare accountants are charged with allocating costs in as precise a manner as possible for each form of healthcare. They also assist in trying to reduce or manage the costs of various mate- rials and activities. This task includes inventory control and uncompensated healthcare. An internal healthcare audit seeks to ensure that accounting and financial operations and state- ments are accurate and that the systems in place protect against intentional or unintentional malfeasance. External audits are imposed by an outside force, such as a government require- ment. Both forms examine a variety of organizational operations and make recommendations for improvements and necessary changes. Key Terms accounts receivable amounts due for all services that have been rendered or items that have been sold for which payment has not yet been made activity-based costing setting prices for healthcare services based, in part, on the level of expertise and precision required capital budget a finance and accounting instrument that assists in planning for major expen- ditures and in acquiring the funds needed to finalize such purchases and lease arrangements cost-plus pricing a pricing approach that adds a fixed amount to the total cost of a product or service
- 54. direct cost healthcare cost that can be attributed to a specific treatment format for a patient or activity financial governance management of two primary responsibilities: (1) oversight of day-to-day operations that require financing and (2) planning for and implementing long-term financial needs fixed cost incurred expense that is not affected by the volume of sales or revenues indirect cost healthcare cost that cannot be attributed to a specific patient or form of service markup pricing a pricing approach that assigns a percentage to add to the total cost per item Critical Thinking Chapter 6 operating budget finance and accounting instrument that maps expected revenues and allo- cates funds to individual departments and activities for their expenses, normally over a one- year period uncompensated healthcare a situation in which uninsured individuals receive medical treat- ment but cannot pay for it or in which others fail to pay their portion of the expense, such as coinsurance
- 55. variable cost cost directly related to volume or revenue working capital a comparison of an organization’s current assets to its current liabilities Additional Resources American Accounting Association http://www.aaahq.org Federation of Schools of Accountancy http://www.thefsa.org Financial Management Association International http://www.fma.org Institute of Management Accountants http://www.imanet.org International Federation of Accountants http://www.ifac.org Management and Accounting Web (database of articles pertaining to management and accounting) http://www.maaw.info National Association of State Boards of Accountancy http://www.nasba.org Critical Thinking Review Questions 1. What two activities are involved in financial governance? 2. What three financial instruments do financial officers use to examine an organization’s monetary well-being? 3. Define working capital. 4. How do managers calculate the amount of working capital an organization holds? 5. Define fixed costs, variable costs, and total costs.
- 56. 6. Define markup pricing and cost-plus pricing. 7. What is a break-even point? 8. What are the advantages and disadvantages of bonds as financial instruments? 9. What are the advantages and disadvantages of loans as financial instruments? 10. What are the advantages and disadvantages of common stock as a financial instrument? 11. What are the advantages and disadvantages of leasing as a financial instrument? 12. What are the differences between a capital budget and an operating budget? 13. What elements are included in accounts receivable management? 14. What are direct and indirect costs in healthcare operations? 15. What is uncompensated healthcare? http://www.aaahq.org http://www.thefsa.org http://www.fma.org http://www.imanet.org http://www.ifac.org http://www.maaw.info http://www.nasba.org Critical Thinking Chapter 6 Analytical Exercises 1. A healthcare organization has $250,000 in the bank, $500,000 in accounts receivable, and $100,000 in on-hand medical supplies. The value of its building is $1,400,000, and the medi- cal equipment on hand is worth $700,000. The organization
- 57. owes $150,000 in accounts payable. The mortgage for the building has a $900,000 balance. The organization also owes $400,000 for its medical equipment on a bank note. Based on these figures, calculate this organization’s amount of equity. 2. An independent physician’s practice earned $975,000 in the past year. The physician paid $50,000 for all supplies. Rent for the physician’s office space was $60,000 for the year. Office salaries totaled $300,000. The physician received a one-time payment of $100,000 for an office building that she had previously owned. Her income tax rate is 40%. Calculate the NIAT for this medical practice. 3. A skilled nursing facility has $450,000 of current assets on hand. The organization has $150,000 in current liabilities on the books. Calculate the organization’s level of working capital. 4. Which pricing method do you believe is most appropriate for the following types of organizations? • Dental surgeon providing intricate procedures • Skilled nursing facility for those with moderate medical needs • Drug store selling over-the-counter medicines and pharmacy drugs • Pharmaceutical company creating new drugs 5. How would a break-even analysis be valuable to the accounting department of a nonprofit hospital operated by a religious group?
- 58. 6. A local for-profit mental health center’s management team is considering the purchase of a building that could be used as a lockdown facility for patients requiring careful, 24-hour scrutiny, such as those at risk of suicide. The building has a life expectancy of 20 years. What form of financing should be used to acquire the building? What method of depreciation should be used? Would your answer change if the managers knew that several major costs would occur in about seven years, including providing a new roof and upgrading the plumb- ing system? Why or why not? 7. How would management views of uncompensated care differ in a for-profit healthcare pro- vider as opposed to a nonprofit healthcare provider? Marketing and Competitive Strategies and Tactics Chapter Objectives After reading this chapter, you should be able to 1. Describe the nature of marketing. 2. Apply strategic marketing concepts to the healthcare industry. 3. Create tactical activities that support the strategic health marketing program using mar-
- 59. kets, products, pricing, and promotions. 4. Develop tactical activities that support the strategic health marketing program using alternative methods, image building, and public relations tools. 5 © Age_fotostock/SuperStock Marketing and Competitive Strategies and Tactics Chapter 5 It may seem odd, or even distasteful, to think that healthcare organizations should mar- ket themselves. The reality is, however, that consumers have many choices as they think about healthcare. Consequently, individual physicians, groups of medical specialists, rehabilitation cen- ters, hospitals, public health organizations, pharmaceutical companies, drug stores, elderly care facilities, and others encounter competitive forces that require a response. “Why do hospitals advertise? There is a noble side to it, and also a realistic side,” said Laura Keller, a spokeswoman for St. Louis University Hospital. Keller continued: I don’t think it ever hurts to remind someone that there are lots of choices that you have if you’re dealing with a major health issue. We need to educate the patient, and there are good messages there. On the business side, people need to understand that without
- 60. money we cannot support our mission. (cited in Doyle, 2012) Many critics believe that these advertising practices have little value. According to Dr. Sidney Wolfe, director of the health research group at Public Citizen: “Hospitals seem to be spending money left and right trying to get more patients. Absent significant cost controls, there’s nothing to stop them. . . . It’s siphoning money away from healthcare. Advertising shouldn’t be confused with taking care of patients or improving patient care” (cited in Doyle, 2012). Samuel Steinberg, a Florida-based hospital finance consultant, also remained skeptical about the bene- fits of advertising: “It’s very difficult to be able to demonstrate that these things are worth the investment. . . . Hospitals and health systems that put a lot of money into advertising say it is beneficial. But when you ask them to prove it, there’s a real short- age of good research that verifies that it’s worth it.” But the Missouri Hospital Association created the following response: “Marketing and advertising is core to our mission to educate the pub- lic, [including] promoting better public health by reminding patients of the need for preventive screenings such as mammograms” (cited in Doyle, 2012). In this era of the proliferation of medical advertising for such things as Viagra and Cialis, jokes
- 61. are made, and complaints are raised. Are pharmaceutical companies and others creating illnesses just to sell medicines for such things as “restless legs syndrome”? Can a line be drawn outlining what is ethical and what is indefensible? This chapter examines healthcare marketing in terms of strategic and tactical decisions and activities designed to maintain the well-being of a practice or organization. The first section explores the basic nature of marketing, followed by a section on strategic marketing concepts. Then, specific strategic marketing activities are presented. The chapter concludes with a descrip- tion of the process of matching marketing tactics with marketing strategies. © Julio Cortez/Associated Press ▲▲ Should healthcare organizations engage in advertising programs? The Nature of Marketing Chapter 5 5.1 The Nature of Marketing The American Marketing Association (AMA) serves as the primary professional organization for marketing academics and practitioners. In 2007, the AMA presented the following defini- tion: “Marketing is the activity, set of institutions, and processes for creating, communicating, delivering, and exchanging offerings that have value for customers, clients, partners, and society at large” (http://www.marketingpower.com). This definition
- 62. suggests that the goal of marketing should be to develop relationships with an organization’s customers and other publics. This con- cept could also be applied to the nature of healthcare. In the past, however, a more traditional definition (Armstrong & Kotler, 2012) for marketing has been: 1. Discovering consumer needs and wants 2. Creating the goods and services that meet those needs and wants 3. Pricing, promoting, and delivering the goods and services According to this definition, marketing begins with an understanding of consumer needs and wants. Thus, the foundation of any marketing management program consists of identifying groups of consumers that share a common desire for a good or service. Only then can the goods or services be created and sold. Primary Marketing Activities and Components The traditional definition of marketing implies six major topics, as shown in Figure 5.1. Figure 5.1 Healthcare marketing Markets (patients as consumers) f05.01_HCA340 Distribution Products
- 63. (goods and services) Pricing Promotion People The Nature of Marketing Chapter 5 Markets consist of people (or businesses) with wants and needs, financial resources, and the will- ingness to spend those resources to satisfy their wants and needs. The most common method for discovering individual markets is to divide them into various consumer and business-to-business segments. In healthcare, however, methods used to identify markets differ from standard for-profit operations. Although most hospitals feature a community or regional focus, many hospitals and smaller healthcare operations also specialize in the treatment of certain illnesses (cancer, heart disease, mental health) or try to reach certain categories of patients (athletes, pregnant women, children, elderly). These groups have wants and needs that can be specified and documented. Products are the physical goods sold to consumers and other organizations, as well as the services that are offered to individual consumers, other businesses, and the government. Physical goods include both durable goods that last more than one year and nondurable goods with shorter
- 64. uses. In healthcare, an example of a durable good is the medical equipment a person purchases for long-term care, such as a wheelchair. Nondurable goods include convenience items, shopping goods, and specialty products. Convenience items include frequently purchased products that feature low prices. In healthcare, convenience items would include over-the-counter medicines and other low-cost health aids, such as heating pads. Shopping goods require consumers to make some level of effort in their choices and purchases. For example, going to a pharmacy to purchase prescriptions, or deciding to purchase a hot tub or exercise equipment to improve one’s health. Orthodontist care would also qualify as a shopping good, due to the increasing availability of options. Specialty products are sold at unique outlets and require a more concerted effort by the individual consumer to find them and purchase them. Few specialty items are associated with healthcare. Services, the intangible items that are sold to others, constitute the primary form of product that is marketed in healthcare. Examples of health services include ambulance delivery of patients, insurance, and most forms of medical care, including regular physician practices, specialists, nursing home care, dentistry, psychiatric care, and rehabilitation services. Prices of goods and services are normally based on costs, demand and supply, competition, and profit goals. As mentioned earlier, patients, or consumers, rarely know the actual price of a health- care service. Pricing complications arise from methods of
- 65. billing, the type of insurance cover- age, government payments, and provider write-offs. In addition, the healthcare provider, such as a hospital, may offer the exact same service at a price that is vastly different from that charged by other similar organizations (James, 2013). When a healthcare facility provides a new good or service, the organization’s leaders can decide whether they want to use a skimming method, in which the price charged is as high as possible, or penetration pricing, in which the price is set as low as the firm can afford. In the unique setting of healthcare, however, neither strategy seems particularly applicable. Instead, costs are allocated across the number of patients served over time by the item or service. Place, or distribution, involves deciding where, how, and when products will be made available to potential customers. In a standard marketing program, distribution includes a decision about the type of distribution approach that will be used: intensive, selective, or exclusive. Intensive distribution means selling the product in every available location and is often associated with convenience goods. Selective distribution involves placing products in outlets that are believed to be profitable or that project a certain image, and not using other outlets. Exclusive distribution restricts the availability of the product to a highly select group of outlets—normally only one per geographic region. The Nature of Marketing Chapter 5
- 66. Some healthcare products that feature intensive distribution are daily or regular-use products, such as aspirin, dental rinse, or a toothbrush. Selective distribution in healthcare occurs when a small number of physicians provides a specific service, such as physical rehabilitation, in a given area. Hospitals tend to operate single locations or a central facility with additional satellite sites. Many types of healthcare services are distributed exclusively, in that only one provider operates in a geographic area. The second activity associated with distribution is the physical distribution program, which involves choosing methods of transportation, types of warehouses, forms of inventory control, and methods of billing and payment. These processes apply to medical suppliers that provide products to larger health facilities. Promotion, another major component of marketing, includes creating and supporting advertis- ing programs, consumer and trade promotions programs, personal selling tactics, and public relations efforts. The most recent trend in promotion involves carefully combining all of these elements into an integrated marketing communications plan (Clow & Baack, 2014). Promotional activities have been strongly influenced by the availability of new alternative media outlets. Traditional advertising and promotional programs have been adapted in response to new tech- nologies and new methods of making contact with customers. The final, and perhaps most critical, component of effective
- 67. marketing is people. In a service industry, such as healthcare, the people performing the services play crucial roles. To a manufac- turer of major medical equipment, the people who operate the machines, deliver the products, and design the marketing program are the key. In a nonprofit operation, the people providing the services to the public, along with the volunteers who help, are the ones who make the organiza- tion successful. Without people, an organization cannot continue to survive. In recent years, customer satisfaction and customer retention have received a great deal of atten- tion. Numerous articles and books focus on what a company or organization should do to achieve customer satisfaction and customer retention. Most of this information can be summarized by these words: product quality and customer service. Without product or service quality, there is no customer satisfaction and no customer retention. Without customer service, the importance of product quality quickly diminishes. Thus, these factors are key components in the healthcare industry (Clow & Baack, 2010). Strategic Marketing and Healthcare In the area of planning, marketing strategies outline the services to be offered and the tar- get markets for those services. Marketing strategies provide broad sweeping plans based on an organization’s mission and vision statements, as described in Chapter 4. The mission statement expresses the primary reasons for the formation and operation of an organization. The vision
- 68. statement outlines the organization’s intended future and offers direction about where the orga- nization seeks to go and what executives hope the organization will become and achieve. These two statements outline the most general direction for the marketing department and program. Together, an organization’s mission statement, vision statement, and marketing strategies outline its key values. Marketing tactics include all of the midrange or medium-term (one- to three-year) efforts designed to support marketing strategies. Many product design issues are tactical issues. In Strategic Marketing Activities Chapter 5 standard marketing programs, tactics include changing the product’s packaging or label, revising or creating new advertising taglines, and improving the methods used to support promotional efforts. Marketing tactics vary across healthcare organizations, as many organizations seek to strengthen a specific brand and engender high levels of confidence regarding the quality of care they provide. Often, healthcare marketing tactics involve public relations efforts, including vari- ous programs that raise awareness of health concerns and teach preventive care. Although most midlevel marketing managers are not involved in developing marketing strategies, they can be heavily involved in creating and implementing marketing tactics.
- 69. Operational plans, or short-term plans, are created to carry out marketing strategies and tactics. Typical short-term plans include departmental budgets, projects, and programs, such as plans for the marketing department’s day-by-day activities. A marketing budget establishes a financial map outlining the amount of money available for the program and how funds will be spent, such as for advertisements, promotional programs, website development and maintenance, and other more routine activities. Projects, or single-use plans, are short-term plans created for one-time activi- ties. An example of a project is a plan for a one-time health seminar on a specific topic. Once the seminar has been held, the project plan is complete. Another project could be the renovation and upgrading of a specific medical service area, such as an operating room. A program consists of a set of projects that leads to a permanent new course of action. An example of a marketing pro- gram is the entire process surrounding the development of a new medical service. The projects associated with that marketing program include developing the service, potentially choosing a name or a brand for that service, creating an advertising program to inform the community of its existence, and other activities (Ferrell, 2013). 5.2 Strategic Marketing Activities Strategic marketing and strategic management overlap in many areas. Effective healthcare administration requires that the two efforts mesh in order to achieve the organization’s strategic and marketing communication objectives. In Chapter 4, strategic management was described in terms of:
- 70. • Analysis and diagnosis—strengths, weaknesses, opportunities, threats (SWOT) analysis • Generating strategic alternatives • Strategy evaluation and choice • Strategy implementation To complement these activities, marketers begin by conducting a supporting program known as a strategic marketing analysis. Strategic Marketing Analysis A strategic marketing analysis program consists of an environmental analysis; a competitive and industry analysis; a segmentation, targeting, and positioning analysis; and a customer analysis (Clow & Baack, 2010). The program also combines elements of a SWOT analysis in that it assesses the external environment and various internal company operations. However, a strategic mar- keting analysis focuses less on strengths, weaknesses, opportunities, and threats, and more on the discovery of how the organization interacts with its environment, its markets, and specific customers. Executives seek to gauge how organizational leaders can create new relationships with Strategic Marketing Activities Chapter 5 patients and customers while also building on current relationships. Such an analysis can be extremely helpful to marketing managers in a healthcare system.
- 71. Environmental Analysis An environmental analysis begins with careful monitoring of all external variables that have an impact on the healthcare industry. Assessments of all political, social, economic, technological, and semicontrollable forces should be made, much in the same format as a SWOT analysis. The information gathered should reflect specific issues that affect healthcare marketing programs, rather than overall strategic implications. For example, when examining political forces, marketers look to laws that directly apply to vari- ous activities, such as advertising. They must become familiar with what can, and what cannot, be said in a commercial for a hospital. The term puffery, for instance, means that an organization can make untestable claims, such as that a hospital is the “friendliest” or that it offers “the most compassionate care,” as no method can be used to verify or disprove such statements. Healthcare marketers also consider shifting demographics, cultural trends and changes, and ris- ing educational levels to assess the impact of the marketing on their intended programs. Economic forces include economic conditions and how these might affect consumer choices, such as the decision to have an elective surgery to improve one’s appearance. Healthcare marketers are con- sistently asked to get the word out regarding new services, service improvements, improvements in the delivery of those services, and technological advancements in medical care. Competitive and Industry Analysis
- 72. A competitive or industry analysis first identifies the levels of competition, from the closest and most intense competitors to those that are the most distant but that are still viable organizations able to take away customers (patients). Marketers investigate each competitor in order to under- stand both the methods used by competitors and the individuals these competitors seek to reach. In healthcare, competition takes various forms. Marketers consult with other top managers to understand the impact on an overall organization, such as a hospital, or a specific form of care, such as an addiction treatment program. Competition arises from other hospitals, alternative care facilities, specific illness treatment centers, and, at times, individual physi- cians. Healthcare is unique in that patient “customers” may be anything from entire companies providing wellness programs to the government, through Medicare and Medicaid programs. Segmentation, Targeting, and Positioning Analysis The segmentation, targeting, and posi- tioning analysis, or STP analysis (Kotler & Armstrong, 2007), helps the marketing team meet the goal of optimizing revenues by reaching the proper audience, both in terms of the services offered and the meth- ods used to contact the individuals who © Jupiterimages/Comstock/Thinkstock ▲▲ In healthcare, one target market might be elderly people.
- 73. Strategic Marketing Activities Chapter 5 might require such services. Segmentation involves identifying all potential customer groups that are viable for the purposes of marketing products and services. Most healthcare organizations cannot create enough services to reach every available type of patient. Thus, a market segment analysis categorizes customers into groups and identifies the characteristics of members of the groups (Myron & Truax, 1996). In traditional marketing programs, a segmentation analysis includes demographic characteris- tics, psychographic variables, behavioral actions, and geographic location. In healthcare, other categories, such as illness type and patient characteristics (some of which are demographic, such as seniors, children, and women), are more useful. The segments can be examined for potential to increase revenues based on the match of the service to the local community, the size of the seg- ment, growth potential, reachability, consumer responsiveness, retention potential, and levels of competition. For example, a local hospital could decide to provide a mobile magnetic resonance imaging (MRI) unit to travel around a county or specified geographic region. A market segment analysis would reveal whether sufficient need exists to justify such a purchase and the employ- ment of specialists to operate the equipment. After segmentation, the targeting component of the STP
- 74. approach can proceed. Targeting includes selecting the market segments (e.g., diseases or groups of patients) that the organization intends to target or reach. For example, a mobile MRI unit would target various injuries, includ- ing those related to sports, accidents, and the aging process. Positioning involves creating perceptions in the minds of consumers about the nature of the orga- nization, its brand, and its products and services. Positioning must match the characteristics of the selected target markets. Continuing the example, a mobile MRI operation would be positioned as a high-quality method of diagnosing injuries that would ensure the best possible care. Marketing programs would note that MRI imaging is superior to X-rays and computed tomography (CT) scans, thus granting the physician greater precision in diagnosing and treating an injury. A positioning analysis discovers the place of an organization and its services in the minds of consumers and relative to the competition. Four components to be considered during this part of the STP analysis include the target audience, the organization itself or the service being offered, the frame of reference or category, and points of differentiation or uniqueness. Once completed, positioning strategies may be put in place. A perceptual map may assist in identifying the position of a healthcare organization in com- parison to the competition. A perceptual map typically employs two axes representing the key variables that affect perceptions of a service. In traditional marketing, price and quality serve
- 75. as the two axes. Figure 5.2 provides a perceptual map containing various providers of the same service—psychiatric care—using two common healthcare factors: affordability and accessibility. Affordability measures the degree to which a patient believes he or she can reasonably pay for healthcare services. Accessibility measures perceptions that a patient could obtain the needed service from a specific healthcare provider. These two concepts can be combined as surrogates for price and then be compared with perceptions of quality to provide a useful analysis. As shown, an individual psychiatrist is perceived as being the least affordable and accessible (the highest price), even though the psychiatrist might be perceived as providing the highest level of care. An individual psychologist costs less and would be more accessible; however, the quality of care might also be viewed as being somewhat lower. (Remember, however, that a patient would be able to examine insurance coverage to see if this changes the costs of each.) A support group Strategic Marketing Activities Chapter 5 in a hospital probably would be reasonably affordable and accessible (moderately priced) and would only hold an advantage over an unlicensed counselor if perceptions were that the quality of care was better. The unlicensed counselor would be perceived as being the most affordable and accessible (lowest price) but may be perceived as providing the least effective quality of care. More
- 76. precise perceptual maps would incorporate the names of specific psychiatrists and psychologists. A quality STP analysis allows an organization to avoid brand parity, or the perception that ser- vices provided by other institutions or physicians are basically the same. Healthcare organiza- tions are best served when marketers are able to build brand equity, or the perception that a given provider is different and better (Schultz, 2009). Any dentist or physician holding such an advantage probably has a highly successful practice, as would any practice group or hospital. Customer Analysis A quality customer analysis provides marketers with an in-depth understanding of an organiza- tion’s customers, or patients in the healthcare system. The “W’s” and “H’s” of a customer analysis include understanding the who, what, when, and where of patients seeking medical services, as well as how those services are obtained. In other words, marketers should ask, “Who are our patients? What services do they seek? When do they seek them (e.g., emergency vs. routine visit)? Where are they located? How are the services obtained?” The answers to these questions help a marketing manager in healthcare establish a target audience to reach. An effective marketing program necessitates careful study of the consumer buying decision- making process for purchasing a service (Clow & Baack, 2014, pp. 53–81). Each step offers the potential to reach and attract customers. Figure 5.3 details the steps of a purchasing process, as
- 77. modified to fit healthcare circumstances. Figure 5.2 A perceptual map for psychiatric care f05.02_HCA340 Affordability and Accessibility (Price) High Quality Low Low High Unlicensed counselor Individual psychiatrist Individual psychologist Hospital-guided support group Strategic Marketing Activities Chapter 5 Consider a person who experiences blurred vision. The individual recognizes that her eyesight has deteriorated. She considers the services of an individual optometrist, an individual ophthal- mologist, or a company such as Pearle Vision Center, which offers both an eye exam and subse- quent fulfillment of an eyeglass prescription. Next, she reviews her healthcare coverage to find out whether eye exams and glasses are included, which would
- 78. affect her subsequent choice. If she is poor or unemployed or if her policy does not cover eye care, she may consider a public health facility that offers eye exams for free. When the patient evaluates alternatives, she considers the cost of each option, along with the level of care. If she worries that a new problem has emerged, such as glaucoma, she may wish to see a more advanced medical professional, depending on the type of insurance she has. If she believes it is simply a matter of obtaining a new prescription, other options become viable. A person with no or low income will also think about the amount of time she would wait in a public health facil- ity and whether she might have to take time off from work to take advantage of the free service. After she makes her choice and resolves the problem, she will review her experience. If she spent a long time in a waiting room and encountered a terse, distant eye care professional, she may tell others not to go to such a place. If her vision does not improve or is not corrected, postpurchase dissatisfaction will be high. She might decide to post her story on social media and websites that evaluate various eye care providers to tell friends and family about the episode. Figure 5.3 The consumer purchasing decision process: Applications to healthcare f05.03_HCA340 Step 1: Problem recognition Recognize a health Issue
- 79. Step 2: Information search Examine potential healthcare providers and options that could resolve the health issue Step 3: Evaluation of alternatives Consider the advantages and disadvantages of each type of healthcare provider Step 4: Purchase decision Seek medical care Step 5: Postpurchase evaluation Consider recovery, degree of wellness, satisfaction with provider Strategic Marketing Activities Chapter 5 In recent times, many healthcare organizations take into consideration the steps of the buying process in some form, with particular atten- tion paid to postpurchase evaluation. A variety of techniques may be used to ascertain levels of patient satisfaction with the services and service providers. Additional Factors When considering customers and patients, healthcare administrators can benefit from meth- ods that help them understand market potential and market demand. Market potential consists of the total number of patients that might require a
- 80. medical service. Market demand is the total cur- rent existing demand for the service. Company or brand demand expresses the demand for a particular company’s brand and is often referred to as market share. For instance, an organization that provides CT scan services can determine how many patients from a geographic area would need scans in the coming year. Then the organiza- tion’s marketers could identify the percentage of patients that use a specific facility as compared with all other facilities. In addition, the concepts of share of mind (awareness and recall) and share of heart (loyalty and affection) provide helpful ideas about how customers view a healthcare organization and its services. In a manner similar to a perceptual map, these two indicators can serve as axes used to evaluate an operation. Figure 5.4 provides an analysis of share of mind and share of heart (Goodall, 2011) for four hospitals in a large metropolitan area. © FogStock/Thinkstock ▲▲ A woman needing new eyeglasses would undergo the purchasing decision-making process. Figure 5.4 A share of mind/share of heart analysis of healthcare facilities f05.04_HCA340 Share of Heart High