Downloaded 570 times
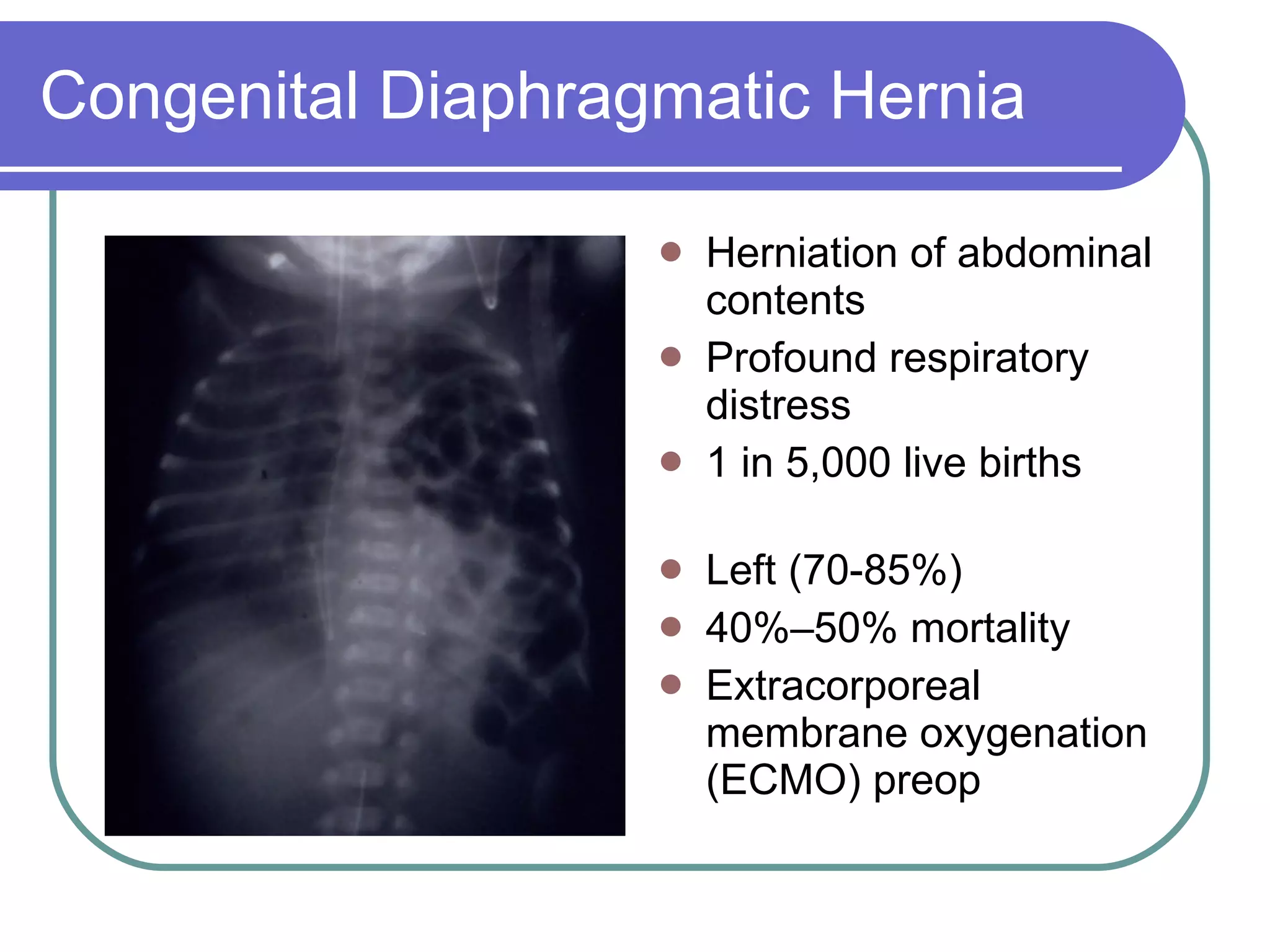
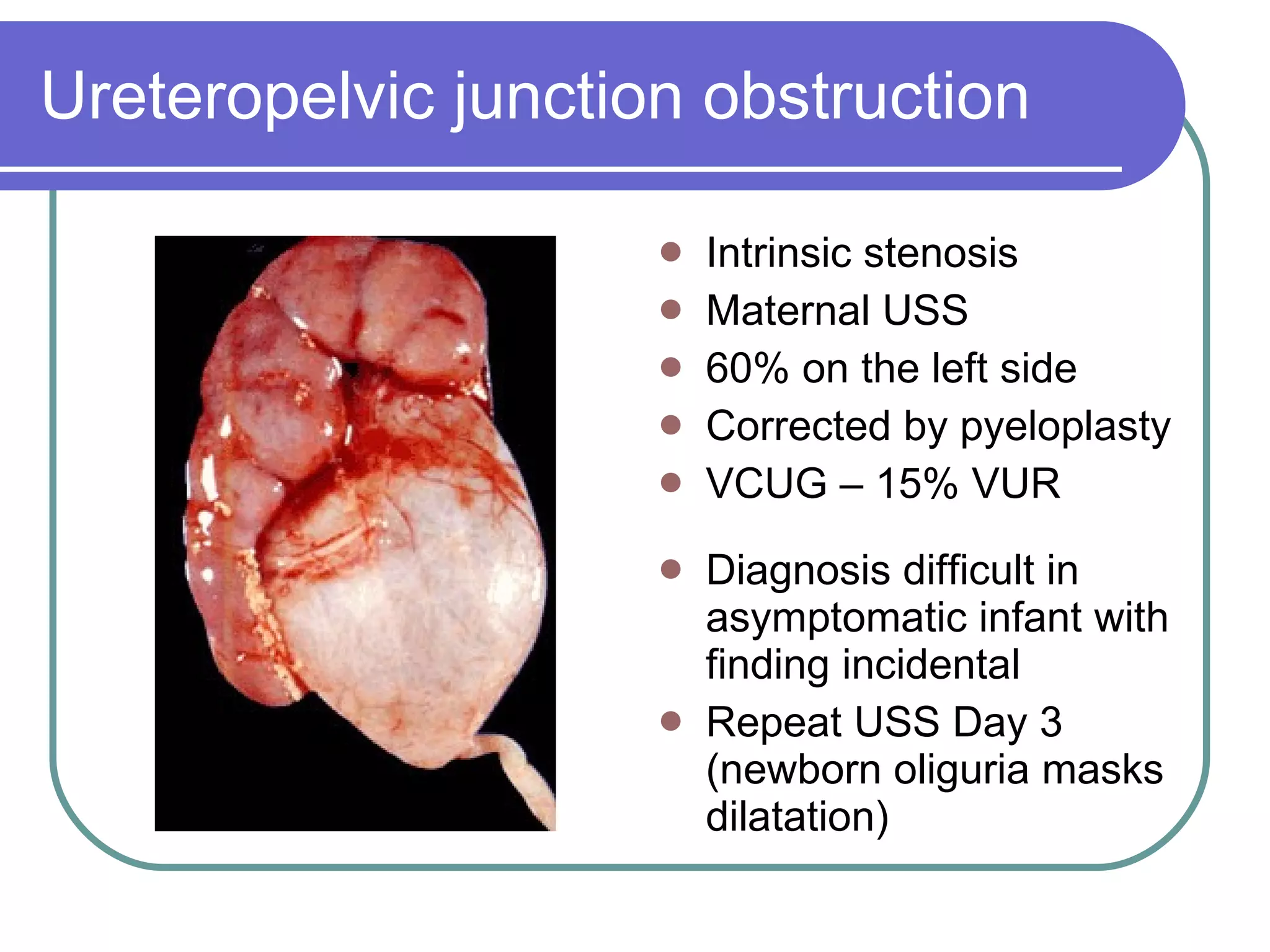
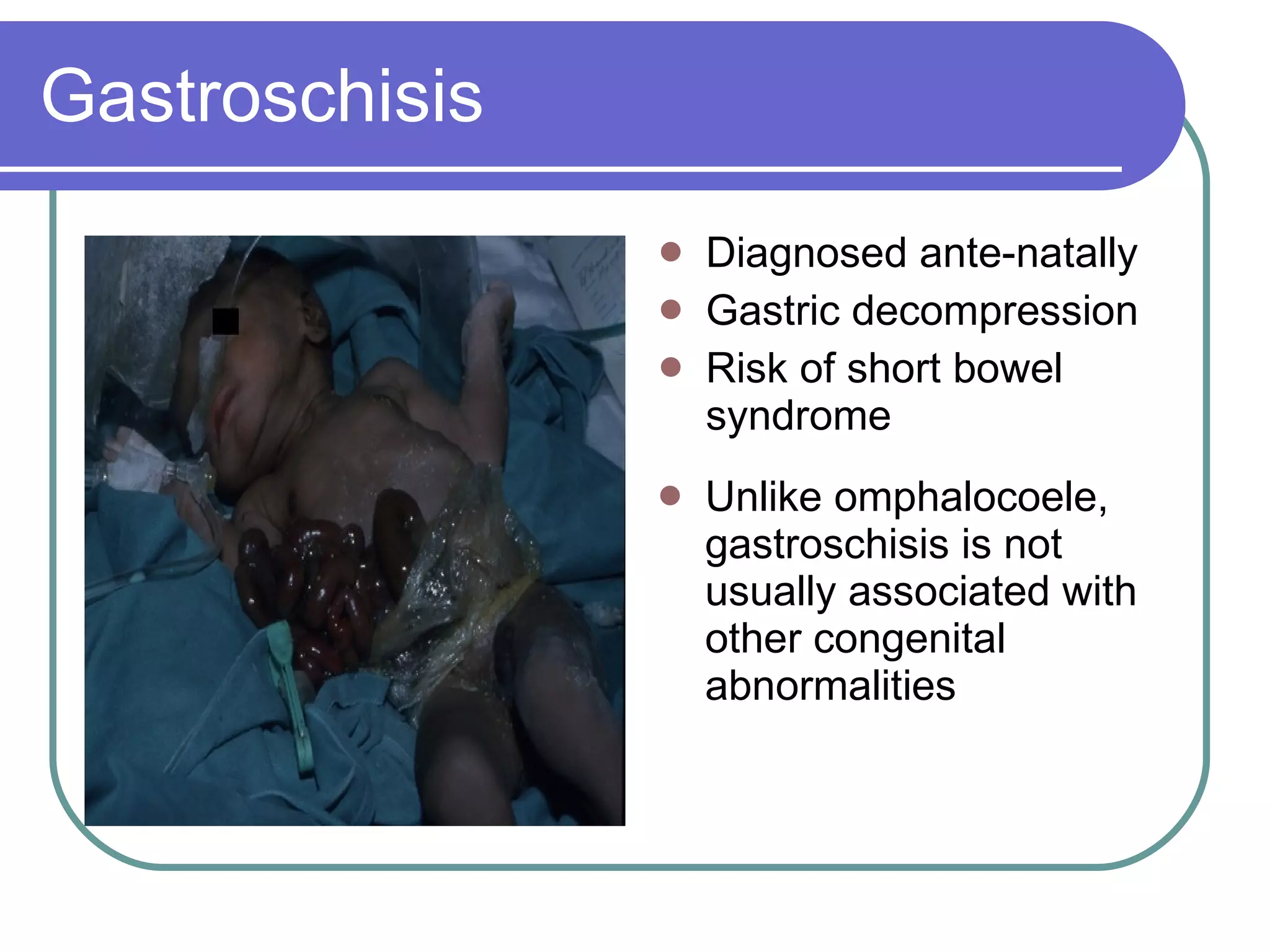

This document discusses several common postnatal and neonatal problems, including: 1) Congenital diaphragmatic hernia, which causes profound respiratory distress in 1 in 5,000 live births. 2) Ureteropelvic junction obstruction, which is often detected incidentally and can be corrected by pyeloplasty. 3) Gastroschisis, which is diagnosed prenatally and carries risks of short bowel syndrome.












































































