
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Update in Central Neuraxial Blockade in Pediatrics
Similar to Update in Central Neuraxial Blockade in Pediatrics (20)
More from cairo1957
Recently uploaded
Recently uploaded (20)
Update in Central Neuraxial Blockade in Pediatrics
- 1. Update in Central Neuraxial blockade in Pediatrics by Hytham Khaled Abou El-Fotouh Assistant lecturer of Anesthesia & Intensive care Faculty of Medicine - Zagazig University
- 2. Contents - Introduction. - The important anatomical differences between pediatrics and adults vertebral column with their central neuraxial block implications. - The Important physiological differences between pediatrics and adults with their central neuraxial block implications. - Indications of CNAB. - Contraindications of CNAB. - Preoperative management. - Measures for patient safety during establishment of CNAB. - Technical procedures. - Advantages. - Disadvantages. - Complications. - Conclusion.
- 3. Introduction: - Neuraxial blockade entails interruption of neuronal transmission at the level of the neuraxis (i.e. the spinal cord) by means of local anesthetic drugs. - They provides adequate intra and postoperative analgesia When combined with general anaesthesia, it reduces the requirement of anaesthetic and analgesic agents. - It is a simple technique, but it has some rare potential life threatening complications as Local anaesthetic toxicity. - To perform these blockades safely in pediatrics, it is mandatory to know the anatomical and the physiological differences between pediatrics (especially neonates and infants) and adults with their central neuroaxial block implications.
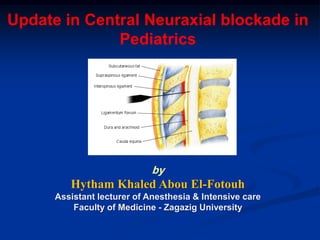
- 4. The important anatomical differences between pediatrics and adults vertebral column with their central neuroaxial block implications: a- The spinal cord reaches: - L3-4 in the neonates and below 1 y old infants. - lower border of L1 (the adult level) at 1y old. So, lumbar puncture for subarachnoid block in neonates and infants should be performed at the L4-L5 or L5-S1 interspace to avoid needle injury to the spinal cord. b- Thoracic spinous processes in neonates and infants are more horizontal in position but with older ages they become more oblique, so - In less than 1 year of age, the needle insertion is perpendicular to the spinous process line. - In older ages the needle insertion acquires cephalic orientation (up to a 45-degree angle to the skin). Fig. (1): Shows the end of both spinal cord and dural sac beside the shape of sacrum, in pediatrics and adults.
- 5. b- Sacrum: - Shape and fusion: - In comparison with adult, the sacrum in infant and young children is flat not fused and consists of five distinct vertebrae (fig.1). - This allows an easy sacral inter-vertebral approach. - The dural sac reaches: - S3-4 in the neonates and below 1 year old infants. - S1-3 (The adult level) at 1 year old. so, there is great liability to accidental intrathecal injection Fig. (1): Shows the end of both spinal cord and dural sac beside the shape of sacrum, in pediatrics and adults. with caudal extradural blockade in below one years old patient than adults. - The sacral hiatus is situated : - Near the natal cleft in adults. - Much higher in infants. - At the middle of sacrum in neonates. - Epidural fat: - Less fibrous in pediatrics (up to 6-7 years of age) so, spread of LA and catheter insertion is easy. The important anatomical differences between pediatrics and adults vertebral column with their central neuroaxial block implications (Cont.):
- 6. c- Tuffier's line level ( the line that joins both anterior superior iliac spinous processes): - Due to delayed ossification and growth of iliac crests: - It crosses the spine at L5-S1 inter-space in infants. - It crosses the spine at L4-L5 inter-space in adults. d- Ligamentum flavum: - It is much thinner and less dense in infants and children than in adults. - This makes the engagement of the epidural needle more difficult to detect and unintended dural puncture during epidural catheter placement a greater risk for the infrequent operator. The important anatomical differences between pediatrics and adults vertebral column with their central neuroaxial block implications (Cont.):
- 7. The Important physiological differences between pediatrics and adults with their central neuroaxial block implications: - Neonates, infants and children are uncooperative, so heavy sedation or general anesthesia is required before establishment of regional blockade. - Nerve fibers in neonates and young children are - Thinner. - Have less myelin This makes neonates, infants and children more sensitive to the effects of local anaesthetics with subsequent rapid onset. So, diluted local anesthetic is as effective as more concentrated anesthetic in adults
- 8. - Cerebrospinal fluid (CSF) volume as a percentage of body weight is greater in infants and young children. So, comparatively larger doses of local anesthetics required for surgical anesthesia with sub- arachnoid block in infants and young children. Figure (2): Approximate volume of cerebrospinal fluid (CSF) relative to weight and age - The CSF turnover rate is greater in infants and children with subsequent much briefer duration of subarachnoid block with any given agent. The Important physiological differences between pediatrics and adults with their central neuroaxial block implications (Cont.):
- 9. The Important physiological differences between pediatrics and adults with their central neuroaxial block implications (Cont.): - Attachment of spinal nerve sheaths in neonates and young children is loose and this leads to leakage of LA along spinal nerve roots during epidural blockade with subsequent the need to large volume of local anesthetic to compensate for this leak along spinal nerve roots. - The incidence of LA toxicity in neonates and infants is higher especially with repeated LA administration due to: : due to large volume of distribution andProlonged elimination ½ life- impaired renal function. : larger amount of free drug.Lower albumin concentrations- : due immature hepatic metabolicDiminished metabolic clearance- pathway and renal function (reach adult levels by 3-5 months of age). that leads to Increased regionalIncreased cardiac output and heart rate- blood flow with subsequent increased systemic absorption of local anesthetic. - The incidence of apnea in neonates are at greatest following opioids caudal extradural administration because of: - Morphine clearance in neonates is one quarter that of adults. - Immature respiratory centre.
- 10. Indications of CNAB: a- For providing anesthesia and analgesia in Lower abdominal and Lower extremity surgery (hip, leg and foot surgical procedures). b- For providing post operative analgesia: - It is established at the end of operation and before recovery from GA to provide post-operative analgesia (continuous infusion method). c- As an adjuvant to GA: - For surgical procedures below the umbilicus. d- For pre-emptive analgesia: - It is established before start of surgical procedures under GA to avoid post operative pain.
- 11. Contraindications of CNAB: A- Absolute: - Parents refusal. - Coagulopathy. - Therapeutic anticoagulation. - Skin infection at injection site. - Raised intracranial pressure Accidental dural puncture in a patient with raised ICP may lead to brainstem herniation (coning). - Hypovolaemia to avoid profound circulatory collapse. - History of allergy to LA. B- Relative: - Pre-existing neurological disorders: such as multiple sclerosis, may be a contraindication, because any new neurological symptoms may be ascribed to the epidural. - Fixed cardiac output states. - Myasthenic patient. - Anatomical abnormalities of vertebral column such as spina bifida, meningomyelocele or scoliosis. - Prophylactic low dose heparin.
- 12. Preoperative management: - Pre-operative visit to: - A formal pre-anaesthetic assessment as prior general anesthesia should be carried out with special considerations to: - The patient's cardiovascular status, especially valvular lesions or other conditions that might impair the ability to increase cardiac output in response to the vasodilatation that inevitably follows sympathetic blockade. - The back should be examined and any lesions or abnormalities noted. - Laboratory assessment of the patient's coagulation status. INR (or prothrombin time), APTT and absolute platelet count should be within the normal range. - Prior to performing the block, all equipment should be checked.
- 13. Measures for patient safety during establishment of CNAB: - The procedure should be conducted in the anesthesia room or theatre . - Stabilizing venous access (to allows administration of intravenous fluids preloading or coloading). - Sedative agents (if required) - Patient monitoring (ECG, BP and SpO2 if sedation is planned). - Drugs and equipments for resuscitation and airway management should be available and ready.
- 14. Techniques for establishment of CNAB: - CNAB are classified according the following: According to the position of needle or catheter insertion it is classified into: - Sacral (Caudal) epidural block. - Lumbar spinal or epidural block. - Thoracic epidural block. - Cervical epidural block. According to the approach: - Median. - Lateral. According to the method of administration of LA: - Single-shot technique - Intermittent bolus. - Continuous infusion technique. According to the combination with spinal or general anaesthesia: - Sole CNAB (cannot applied in pediatrics because they are uncooperative). - Combined with spinal blockade: Combined spinal-epidural. - Combined with general anesthesia: Adjuvant to general anaesthesia.
- 15. Techniques for establishment of CNAB (Cont.): Equipment: - The tray is prepared with the following: - Sterile towels and 4"x4" gauze packs. - Pediatric size spinal or epidural needles Needles should have a clear plastic hub and a small dead space. - 1or 2 syringes (the selected size depends on the calculated LA volume which will be used for blockade). - Marker in case of caudal blockade. - The selected Local anesthetic type and concentration. - Sterile gloves. - Antiseptic solutions. - Plaster. Pediatric epidural Needle sizePediatric spinal needle sizes
- 16. Techniques for establishment of CNAB (Cont.): Identification of epidural space: a- loss of resistance technique. b- Hanging drop technique.
- 17. Techniques for establishment of CNAB (Cont.): Identifications of Sacral Hiatus (SH) for caudal blockade: Methods of identifications of SH: i- Draw an equilateral triangle, the base of which is the distance between posterior superior iliac spines. - The apex of this triangle will point inferiorly over sacral hiatus. ii- The sacral hiatus can be located by: first palpating the coccyx, and then sliding the palpating finger in a cephalad direction (towards the head) until a depression in the skin is felt. iii- Fluoroscopy to locate the sacral hiatus and determination of the optimal angle of needle insertion during caudal block. iv- Ultrasound Guidance to locate the sacral hiatus and determination of the optimal angle of needle insertion during caudal block.
- 18. Techniques for establishment of CNAB (Cont.): Confirmation of Proper Epidural Needle/Catheter Placement: 1- Aspiration. 2- Test dose. 3- Radiographic methods: - X-ray imaging in conjunction with a contrasting agent precisely identifies the tip of the catheter at a specific spinal level. - Fluoroscopy permits the real-time monitoring and adjustment of advancing catheters. 4- Ultrasound-guided techniques: - It allows the real-time visualization of epidural needle tip and catheter placement.
- 19. 5- Epidural electric stimulation test (Recently used): Principle Stimulation of the spinal nerve roots with electrical current conducted through normal saline in the epidural space via an electrically conducting catheter. Sign of correct placement of epidural catheter tip: -Correct placement of the epidural catheter tip (1-2 cm from the nerve roots) is indicated by a motor response elicited with a current between 1-10 mA. Limitations of the use of Epidural stimulation test: - It cannot be performed if any significant neuromuscular blockade is present or local anesthetics have been administered in the epidural space. Figure 1. Epidural electric stimulation test Equipment: The stimulating catheter set-up requires the cathode lead (black for block) of the nerve stimulator to be connected to the epidural catheter via an electrode adapter while the anode lead is connected to an electrode on patient’s skin as the grounding site Techniques for establishment of CNAB (Cont.): Confirmation of Proper Epidural Needle/Catheter Placement (Cont.):
- 20. 6- Epidural ECG technique: - Using epidural ECG, the anatomical position of the epidural catheter is determined by comparing the ECG signal from the tip of the catheter to a signal from a surface electrode positioned at the “target” segmental level. Techniques for establishment of CNAB (Cont.): Confirmation of Proper Epidural Needle/Catheter Placement (Cont.):
- 21. LA dose for various CNAB in pediatrics: a- LA dose for spinal blockade in pediatrics: Local Anesthetic Dose (mg/kg) Volume (mL/kg) Tetracaine 1% 0.4-1.0 0.04-0.1 Tetracaine 1% with epinephrine 0.4-1.0 0.04-0.1 Bupivacaine 0.5% isobaric or hyperbaric 0.5-1.0 0.1-0.2 Levobupivacaine 0.5% 1.0 0.2 Ropivacaine 0.5% 1.08 0.22 - Usual Doses of Local Anesthetics for Spinal Anesthesia in Neonates (up to a Weight of 5 kg) are presented in the following table: Local Anesthetic Usual Dose(s) 0.5% Isobaric or hyperbaric bupivacaine 5 to 15 kg: 0.4 mg/kg (0.08 mL/kg) >15 kg: 0.3 mg/kg (0.06 mL/kg) 0.5% Isobaric or hyperbaric tetracaine 5 to 15 kg: 0.4 mg/kg (0.08 mL/kg) >15 kg: 0.3 mg/kg (0.06 mL/kg) 0.5% Isobaric levobupivacaine 5 to 15 kg: 0.4 mg/kg (0.08 mL/kg) 15-40 kg: 0.3 mg/kg (0.06 mL/kg) >40 kg: 0.25 mg/kg (0.05 mL/kg) 0.5% Isobaric ropivacaine 0.5 mg/kg (max 20 mg) - Usual Doses of Local Anesthetics for Spinal Anesthesia in Children and Adolescents are presented in the following table: Techniques for establishment of CNAB (Cont.):
- 22. Techniques for establishment of CNAB (Cont.): LA dose for various CNAB in pediatrics (Cont.): b- LA dose for epidural blockade in pediatrics: - Up to 10 Kg: 0.2ml/kg increments (0.8ml/kg total). - Above 10 to 25Kg: 0.15ml/kg increments (0.6ml/kg total). - Above 25 to 40Kg: 0.1ml/kg increments (0.4ml/kg total). - Above 40Kg: 0.075ml/kg increments (0. 3ml/kg total to a maximum of 20 ml).
- 23. Techniques for establishment of CNAB (Cont.): LA dose for various CNAB in pediatrics (Cont.): c- Calculation of the appropriate dose of bupivacaine in single shot' technique to provide caudal block for the various surgical levels: 1- According to Armitage: - Armitage recommended the following bupivacaine volume for the various surgical levels: - 0.5 ml/kg for a lumbo-sacral block. - 1 ml/kg for a thoraco-lumber block. - 1.25 ml/kg for a mid- thoracic block. - Also he recommended the following bupivacaine concentration: - For volume up to 20 ml. 0.25% bupivacaine is recommended. - For volume above 20 ml 0.19% bupivacaine is recommended (a part of 0.9% NaCl + three parts of 0.25% bupivacaine = 0.19% mixture). 2- According to Scott : Scott calculates the dose of bupivacaine for various block levels according to child's age or weight.
- 24. Techniques for establishment of CNAB (Cont.): Testing the spread of CNAB : a- Pinprick or touch sensation and cold stimulus with ice. Disadvantages: - These are subjective methods for testing. - Disturbing for the child. b- Transcutaneous electrical stimulation: - It is a precise, reproducible, feasible and inexpensive method for both clinical and research use.
- 25. Advantages of CNAB in comparison with GA: 1- Reduced risk of airway obstruction or the aspiration of gastric contents. 2- Less risk on patients with respiratory disease. 3- Relatively minimal cost. 4- Less risk on diabetic patients. 5- Excellent muscle relaxation. 7- Increase splanchnic blood flow and this may reduce the incidence of anastomotic dehiscence. 8- Rapid return of normal gut function following surgery. 9- less post-operative deep vein thrombosis and pulmonary emboli.
- 26. Disadvantages of CNAB: - Difficult to find the sub-arachnoid or epidural space in some cases. - Associated with some failures. - Liability to unilateral, patchy and too low block level. - Liability to hypotension especially with higher blocks. - Liability to visceral injury. - Not accepted by some parents or surgeons - Single shot CNAB is not suitable for surgery lasting longer than approximately 2 hours. - Relatively it needs long time to perform. - Risk of introducing infection into the extradural or sub- arachnoid space. - Liability to neurologic injury. - Liability to postdural puncture headache.
- 27. Complications of CNAB : Early Complications: - LA toxicity. - Total spinal block - Hypotension. - Bradycardia. - Cardiac arrest . Late Complications: - Neurologic injury. - Visceral injury. - Postdural puncture headache. - Backache. - Infection. - Urinary retention.
- 28. Conclusion: - Central neuraxial blockade in pediatric is relatively a simple technique but it has some rare potential life threatening complications as: - Local anaesthetic toxicity. - High spinal blockade. -- To perform this block safely in pediatrics, it is mandatory to know : - The anatomical and physiological differences between pediatrics and adults with their central neuroaxial block implications. - The correct technical procedures. - The safety measures before LA injections - Beside close monitoring of ventilation, oxygenation, and circulation during and after blockade.