
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Nipah virus
Similar to Nipah virus (20)
Recently uploaded
Recently uploaded (20)
Nipah virus
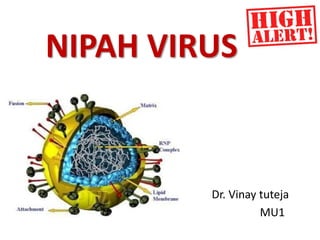
- 1. NIPAH VIRUS Dr. Vinay tuteja MU1
- 3. INTRODUCTION Human Nipah Virus(NiV) infection is an emerging zoonotic disease which causes severe disease in both humans and animals. Nipah virus (NiV) is a member of the family Paramyxoviridae,genus Henipavirus. It was first recognized in Malaysia and Singapore during an outbreak from September 1998 through May 1999. Its name originated from kampung Sungai Nipah, a village in the Malaysian Peninsula where pig farmers became ill with encephalitis.
- 4. Distribution map of pteropus bat EPIDEMIOLOGY
- 5. GEOGRAPHICAL DISTRIBUTION OF OUTBREAKS OF NIV INFECTION IN BANGLADESH AND INDIA
- 6. TRANSMISSION Fruit bats of the genus Pteropus have been identified as natural reservoirs of NiV. Infected bats shed the virus in their excretion and secretions such as saliva, urine, semen and excreta, but they are symptomless carriers. Pigs acquire NiV after contact with infected bats or their secretions or by consumption of raw date palm sap n other fruits contaminated with infectious bat excretions. Pigs act as an intermediate and possibly amplifying host.
- 7. TRANSMISSION IN HUMANS • Direct contact with infected bats, infected pigs, or from other NiV infected people.
- 8. ABOUT THE AGENT NiV is a highly pathogenic paramyxovirus belonging to genus Henipavirus [1]. It is an enveloped negative sense ssRNA virus [2]. SUSCEPTIBILITY TO DISINFECTANTS: Inactivated by 0.1% formalin, and 0.5% household bleach(11). PHYSICAL INACTIVATION: Samples containing Nipah virus diluted in phosphate buffered saline containing Tween-20 and Triton-X100 have been heat inactivated at 56ºC for 30 minutes (12).
- 9. There is strong evidence that the emergence of bat-related viral infection communicable to humans and animals has been attributed to loss of natural habitat of bats.[5] Seasonality was strongly implicated in NiV outbreaks in Bangladesh and India. All of the outbreaks occurred during the months of winter to spring (December-May). Seasonality could be associated with several factors like the breeding season of the bats, increased shedding of virus by the bats and the date palm sap harvesting season.
- 10. The median incubation period of the secondary cases who had a single exposure to Nipah case is 9 days (6–11 days)[6, 7, 8]. The median incubation period following single intake of raw date palm sap to onset of illness is 7 days (2-12 days) [6, 7, 8]. The nucleotide sequences of NiV strains isolated from pigs and persons in Malaysia were remarkably similar and suggest that the entire outbreak was caused by 1 or 2 closely related strains[3]. But recurrent Nipah outbreaks have been recognized since 2001 and the strains of Nipah isolates show substantial heterogeneity in their nucleotide sequences.[4]
- 11. PATHOGENESIS The pathologic findings in the brain of Nipah encephalitis cases showed evidence of necrotizing vasculitis[8]. The main pathology appeared to be widespread ischemia and infarction caused by vasculitis-induced thrombosis, although direct neuronal invasion may also play a major role in the pathogenesis of the encephalitis. Alveolar hemorrhage, pulmonary edema and aspiration pneumonia were often encountered in the lungs [8]. These may lead to pneumonia and acute respiratory distress syndrome (ARDS) ultimately.
- 12. PRPRIMARY VIRUS REPLICATION VIVIREMIA VVASCULAR INFECTION VASCULITIS VIREMIATHROMOSIS & OBSTRUCTION VIREMIAEXTRAVASCULAR SPREAD VIREMIAISCHEMIA & INFARCTION VIRPARENCHYMAL INFECTION AND CELLULAR INJURY
- 13. CLINICAL FEATURES Fever Cough Vomiting Severe weakness Headache Altered mental status Respiratory distress Muscle pain Convulsion Diarrhoea
- 14. DISEASE IN ANIMALS Highly contagious May be asymptomatic Acute fever Severe respiratory disease Barking pig syndrome(characteristic cough) Encephalitis Low mortality
- 15. Relapsed encephalitis: A case is considered to be relapsed encephalitis if the neurological symptoms recur after recovery from encephalitis. Relapsed encephalitis with acute onset of fever, headache, seizures and focal neurological signs occurring months to years after recovery from the initial acute encephalitis. Manifesting in oculomotor palsy and cervical dystonia. Late-onset encephalitis: If the neurological signs and symptoms of encephalitis develop after more than 10 weeks of the initial exposure, it is known as late onset encephalitis.
- 16. DIFFERENTIAL DIAGNOSIS Viral encephalitis (Herpes simplex encephalitis, Japanese B Encephalitis ) Bacterial meningitis Cerebral Malaria
- 17. CASE DEFINITION OF NIPAH ENCEPHALITIS(1) SUSPECTED CASE A person fulfilling both of the following criteria is defined as a suspected case 1. Features of acute encephalitis as demonstrated by a. Acute onset of fever AND b. Evidence of acute brain dysfunction as manifested by i. Altered mental status OR ii. New onset of seizure OR iii. Any other neurological deficit 2. Epidemiological linkage a. Drinking raw date palm sap OR b. Occurring during Nipah season OR c. Patient from Nipah endemic area 1.Surveillance, Prevention and Control of Nipah Virus Infection: A Practical Handbook
- 18. PROBABLE CASE A person with features of acute encephalitis 1.During a Nipah outbreak in the area or 2.With history of contact with confirmed Nipah patient In both suspected and probable cases, the patient might present with respiratory features with or without encephalitis. • The respiratory features are Illness < 7 days duration • Acute onset of fever • Severe shortness of breath, cough • Chest radiograph showing diffuse infiltrates.
- 19. CONFIRMED CASE A suspected or probable case with laboratory confirmation of Nipah virus infection either by: IgM antibody against Nipah virus by ELISA in serum or cerebrospinal fluid Nipah virus RNA identified by PCR from respiratory secretions, urine, or cerebrospinal fluid. Definition of Cluster Two or more suspect cases living within a 30 minute walk of each other who develop symptoms within 21 days of each other.
- 20. CSF study- mild pleocytosis. Normal or slightly raised protein and normal sugar level. MRI of brain- diffuse confluent high signal lesions involving mainly the cortical grey matter and to a lesser extent sub- cortical and deep white matter on T2W and FLAIR sequences. Electroencephalogram: The electroencephalogram (EEG) shows continuous diffuse slow waves with or without periodic bitemporal independent sharp wave discharges. It is important especially to differentiate from HSV encephalitis. [periodic lateralized epileptiform discharges (PLED) mainly from temporal lobe] SPECIAL INVESTIGATIONS
- 21. Enzyme-linked immunoassay The diagnosis of Nipah virus infection can be established by ELISA for CSF & SERUM Nipah IgM capture ELISA and an indirect IgG ELISA have high specificity for the diagnosis. Rapid immune plaque assays have been developed to quantify Hendra and NiV and detect neutralizing antibodies to both viruses. Polymerase chain reaction (PCR) RT PCRs can be used for detection of viral sequences in CSF, throat swab or urine specimens.
- 22. Various outbreaks Location No. cases No. deaths Case fatality (%) Jan–Feb 2001 Siliguri (India) 66 45 68 Apr–May 2001 Meherpur (Bangladesh) 13 9 69 Jan 2003 Naogaon (Bangladesh) 12 8 67 Jan 2004 Rajbari(Bangladesh) 31 23 74 Apr 2004 Faridpur (Bangladesh) 36 27 75 Jan–Mar 2005 Tangail (Bangladesh) 12 11 92 Jan–Feb 2007 Thakurgaon (Bangladesh) 7 3 43 Mar 2007 Kushtia, Pabna, Natore (Bangladesh) 8 5 63 Apr 2007 Naogaon (Bangladesh) 3 1 33 April 2007 Nadia (India) 5 5 101 Feb 2008 Manikgonj (Bangladesh) 4 4 101 Apr 2008 Rajbari and Faridpur (Bangladesh) 7 5 71 Jan 2009 Gaibandha, Rangpur and Nilphamari (Bangladesh) 3 0 0 Jan 2009 Rajbari (Bangladesh)
- 23. Jan 2009 Gaibandha, Rangpur and Nilphamari (Bangladesh) 3 0 0 Jan 2009 Rajbari (Bangladesh) 1 1 101 Feb–Mar 2010 Faridpur, Rajbari,Gopalganj,M adaripur (Bangladesh) 16 14 87.5 Jan–Feb 2011 Lalmohirhat, Dinajpur, Comilla, Nilphamari and Rangpur (Bangladesh) 44 40 91 Feb 2012 Joypurhat, Rajshahi, Natore, Rajbari and Gopalganj (Bangladesh) 12 10 83 Jan–Feb 2013 Gaibandha, Natore, Rajshahi, Naogaon, Rajbari, Pabna, Jhenaidah, Mymensingh (Bangladesh) 12 10 83 Total 292 221 75.7
- 24. OUTBREAKS IN INDIA !!!
- 25. MOST RECENT OUTBREAK: MAY 2018 Perambra town in Kozhikode district. The outbreak started with the death of three members of a family in Perambra in a span of two weeks. Many bats were found to be housed in the well from where the family was drawing water.
- 26. SURVEILLANCE(1) Setting up a surveillance system is important in those countries where there has been an outbreak or evidence of infection in bats. Various types of surveillance for Nipah: Event-based surveillance Case-based (hospital-based) surveillance Surveillance in bats 1.Surveillance, Prevention and Control of Nipah Virus Infection: A Practical Handbook
- 27. TREATMENT There is no effective specific treatment for NiV infection. Treatment is symptomatic and supportive Because NiV encephalitis can be transmitted person-to- person, standard infection control practices and proper measures are important in preventing nosocomial infections.
- 30. Precautions
- 31. • VARIOUS RISK OF TRANSMISSION OF THE VIRUS AND PREVENTION(1) 1. Preventing transmission from bat to human Don’t drink raw date palm sap Consuming boiled sap or molasses is safe 2. Preventing transmission from human to human Wash hands thoroughly with soap and water after coming in contact with patient. Sleep in separate bed. Maintain >1 full-stretched arm distance (1 metre or 3 feet)from patient. Keep personal items of patient separately. Wash used items of patient with soap and water, separately. 1.Surveillance, Prevention and Control of Nipah Virus Infection: A Practical Handbook
- 32. 3. In health care facility Segregate Nipah patients from other patients in the isolation ward/facility. Restrict the number of service providers in the isolation ward. Maintain at least 1 meter (3 feet: one fully stretched arm’s length) distance between two beds for Nipah patient. Admit all cases with fever and unconsciousness/ convulsion/difficulty breathing to the isolation ward/ facility in the hospital. Use mask and gloves during history- taking, physical examination,sample collection and other care-giving to suspected Nipah cases. Avoid unnecessary contact with suspected Nipah cases
- 33. 4. Waste disposal Keep disposable and non-disposable PPEs and items in separate containers/ biohazard bags. Keep sharp wastes in separate designated rigid container (box, bottle etc.). Decontaminate wastes by autoclaving/chemical [Sodium hypochlorite]. Clean and disinfect patient’s room (detergent and sodium hypochlorite) at least once daily specially frequently touched surfaces (e.g. doors, windows, table top, etc). Soak reusable items in 0.05%-0.5% bleach solution or in soap/detergent water for 10-30 min. Autoclave for reuse.
- 34. 5. Handling of deceased body During transportation of dead body from hospital to home, avoid close contact with deceased’s face, especially respiratory secretion. Cover face with a piece of cloth during washing/ritual bath of deceased body. Wash hands with soap, if possible take bath with soap immediately after performing ritual bath of the dead body. Wash reusable items (cloths, utensils, etc.) with soap/detergent and Dry mattress, quilt/comforter, pillow, etc. in sunlight for several consecutive days.
- 38. NIPAH AS A BIOLOGICAL AGENT It is a CDC category c bioterrorism agent Emerging pathogen Potentially high morbidity and mortality. Major health impact Aerosolization potential Economic impact Social disruption (fear,panic)
- 40. REFERENCES 1.Chua, K.B., Nipah virus outbreak in Malaysia. J Clin Virol, 2003. 26(3): p. 265-275. 2. Chua, K.B., et al. Nipah virus: a recently emergent deadly paramyxovirus. Science, 2000. 288 3. Goh KJ, Tan CT, Chew NK, Tan PSK, Chua KB,Lam SK. Clinical features of Nipah virus encephalitis Med. 2000;342 (17): 1229–1235. 4. Paton, N.I., et al. Outbreak of Nipah-virus infection among abattoir workers in Singapore.Lancet 1999. 354(9186): p. 1253-1256. 5. Field, H., et al. The natural history of Hendra and Nipah viruses., 2001. 3(4): p.307-314. 6. Chua, K.B., et al., Isolation of Nipah virus from Malaysian Island flying-foxes. Microbes Infect., 2002. 4(2): p. 145-151. 7. Middleton, D.J., et al. Experimental Nipah virus infection in pteropid bats (Pteropus poliocephalus). J Comp Pathol, 2007. 136(4): p. 266-272. 8. Yob, J.M., et al. Nipah virus infection in bats (order Chiroptera) in peninsular Malaysia. Emerg Infect Dis. 2001. 7(3): p. 439. 9.Hossain, M.J., et al. Clinical presentation of nipah virus infection in Bangladesh. Clin Infect Dis, 2008. 46(7): p. 977-84. 10. Chong HT, H.M., Tan CT. Difference in epidemiologic and clinical features of Nipah viurs encephalitis between Malaysian and Bangladesh outbreaks. Neurology Asia, 2008. 13: p. 23-26. 11.Daniels, P., Ksiazek, T., & Eaton, B. T. (2001). Laboratory diagnosis of Nipahand Hendra virus infections. Microbes and Infection, 3(4), 289-295 12.Sewell, D. L. (2003). Laboratory safety practices associated with potential agents of biocrime or bioterrorism. Journal of Clinical Microbiology, 41(7), 2801-2809.Imada
- 41. Take home message Destroying Nature Unleashes Infectious Diseases !!!! Good food hygiene is great for health. Cont’d
- 42. QUESTIONS Q 1. Nipah virus belongs to which genus? 1. Henipavirus 2. Morbillivirus 3. Respirovirus 4. Rubulavirus
- 43. Q2. Nipah belongs to which category of bioterrorism ? 1. A 2. B 3. C 4. D
- 44. Q3. Chemical disinfection for Nipah virus is done with? 1. Alcohol 2. Sodium hypochlorite 3. Hydrogen peroxide 4. Iodophors
- 45. Q4. Genome of Nipah virus is ? 1. (+) ssRN 2. (-) ss DNA 3. (-) ss RNA 4. (+) ds RNA
- 46. Q5. Most recent drug in development for NiV infection? 1. Ribavirin 2. Tenofovir 3. Retonavir 4. Favipiravir
- 47. THANK YOU !