
Recommended
Recommended
More Related Content
Similar to Costa CPV da, Luz MHBA, Bezerra AKF, Rocha SS da. .docx
Similar to Costa CPV da, Luz MHBA, Bezerra AKF, Rocha SS da. .docx (20)
More from vanesaburnand
More from vanesaburnand (20)
Recently uploaded
Recently uploaded (20)
Costa CPV da, Luz MHBA, Bezerra AKF, Rocha SS da. .docx
- 1. Costa CPV da, Luz MHBA, Bezerra AKF, Rocha SS da. Application of the nursing theory of Callista Roy... English/Portuguese J Nurs UFPE on line., Recife, 10(Suppl. 1):352-60, Jan., 2016 352 ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.7901- 80479-1-SP.1001sup201622 APPLICATION OF THE NURSING THEORY OF CALLISTA ROY TO THE PATIENT WITH CEREBRAL VASCULAR ACCIDENT APLICAÇÃO DA TEORIA DE ENFERMAGEM DE CALLISTA ROY AO PACIENTE COM ACIDENTE VASCULAR CEREBRAL APLICACIÓN DE LA TEORÍA DE ENFERMERÍA DE CALLISTA ROY AL PACIENTE CON ACCIDENTE VASCULAR CEREBRAL Cecília Passos Vaz da Costa 1 , Maria Helena Barros Araújo Luz 2 , Alessandra Kelly Freire Bezerra
- 2. 3 , Silvana Santiago da Rocha 4 ABSTRACT Objective: reporting the experience of application of the nursing process implemented in the light of the Theory of Adaptation of Callista Roy to a patient with stroke. Method: a descriptive study of type experience report, resulting from the application of the nursing process to a patient admitted in a neurological clinic of an emergency hospital in the city of Teresina, Piaui, in 2013. Results: showed itself 15 nursing diagnoses listed based on the taxonomy of the North American Nursing Diagnosis Association International and to establish interventions and nursing results there was used respectively the Classification of Nursing Interventions and the Classification and Nursing Outcomes. Conclusion: facing the findings, Roy's theory contributed to nursing care to patients affected by this pathology by giving importance to the stimuli that trigger responses which require the adaptation of the patient. Descriptors: Stroke; Nursing Theory; Nursing Care. RESUMO Objetivo: relatar a experiência da aplicação do processo de enfermagem implementado à luz da Teoria da Adaptação de Callista Roy a uma paciente com acidente
- 3. vascular cerebral. Método: estudo descritivo, tipo relato de experiência, resultante da aplicação do processo de enfermagem a uma paciente internada em uma clínica neurológica de um hospital de urgência do município de Teresina, Piauí no ano de 2013. Resultados: evidenciaram-se 15 diagnósticos de enfermagem elencados com base na taxonomia da North American Nursing Diagnoses Association International e para estabelecer as intervenções e resultados de enfermagem utilizou-se respectivamente a Classificação das Intervenções de Enfermagem e a Classificação dos Resultados de Enfermagem. Conclusão: diante dos achados, a teoria de Roy contribuiu com o cuidado de enfermagem a paciente acometida por tal patologia ao dar importância aos estímulos que desencadeiam respostas, as quais exigem a adaptação da paciente. Descritores: Acidente Vascular Cerebral; Teoria de Enfermagem; Cuidados de Enfermagem. RESUMEN Objetivo: presentar la experiencia de la aplicación del proceso de enfermería aplicado a la luz de la Teoría de Adaptación de Callista Roy a un paciente con ictus. Método: un estudio descriptivo del tipo relato de experiencia, resultante de la aplicación del proceso de enfermería a una paciente ingresada en una clínica neurológica de un hospital de emergencia en la ciudad de Teresina, Piauí, en 2013. Resultados: se presentaron 15 diagnósticos de enfermería enumerados basados en la taxonomía de la North American Nursing
- 4. Diagnoses Association International y para establecer las intervenciones y resultados de enfermería se utilizan, respectivamente, la Clasificación de Intervenciones de Enfermería y la Clasificación de los Resultados de Enfermería. Conclusión: en los resultados, la teoría de Roy contribuyó a los cuidados de enfermería a los pacientes afectados por esta patología, dando importancia a los estímulos que desencadenan respuestas que requieran la adaptación del paciente. Descriptores: Accidente Cerebrovascular; Teoría de Enfermería; Cuidados de Enfermería. 1 Nurse, Master’s Student, Nursing Postgraduate Program, Federal University of Piaui/PPGENF/UFPI. Teresina (PI), Brazil. Email: [email protected]; 2 Nurse, Master’s Student, Nursing Postgraduate Program, Federal University of Piaui/PPGENF/UFPI. Teresina (PI), Brazil. Email: [email protected]; 3 Nurse, Master’s Student, Nursing Postgraduate Program, Federal University of Piaui. Teresina (PI), Brazil. Email: [email protected]; 4 Nurse, Professor of Nursing, Nursing Postgraduate Program, Federal
- 5. University of Piaui/PPGENF/UFPI. Teresina (PI), Brazil. Email: [email protected] CASE REPORT ARTICLE mailto:[email protected] mailto:[email protected] mailto:[email protected] mailto:[email protected] Costa CPV da, Luz MHBA, Bezerra AKF, Rocha SS da. Application of the nursing theory of Callista Roy... English/Portuguese J Nurs UFPE on line., Recife, 10(Suppl. 1):352-60, Jan., 2016 353 ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.7901- 80479-1-SP.1001sup201622 Through the view of the World Health Organization the patient affected by a chronic disease, such as stroke (CVA), needs planned
- 6. care able to meet his basic needs and provide integrated care, in addition, this condition requires that the same reorganize his daily life, in order to find new ways of relating to life. 1 As the base of nursing process, Nursing offers theories or conceptual models consisting of an organization of central concepts of the profession in an orderly and scientific way to direct data collection, identification of changes in the clinical condition of the patient, the nursing interventions and evaluation of the results. Among these, it emphasizes the conceptual model of the proposed adaptation by Callista Roy, which includes the notion of stimuli and responses. The appearance of stimuli takes
- 7. the need for part of the individual responses for coping mechanisms that are triggered which are processed through two subsystems defined as regulator and knowing. That may be chemical, neural and endocrine, already recognizing that the subsystem is related to higher brain functions of perception, emotion or judgment processing of information. 2-3 The resulting behaviors of these subsystems are observed from four adaptive modes. In physiological way the person responds like a physical environmental incentives and involves five basic needs of physiological integrity (oxygenation, nutrition, elimination, activity and rest, and protection) and four complex processes (sensory, fluid and electrolytes, neurological function and function endocrine).
- 8. The self-mode focuses on the psychological and spiritual aspects of a person and includes self-physical (includes sensation and body image) and self-personnel (includes self- consistency, self-ideal and self-ethical-moral- spiritual). 2-4 But the function mode/role performance focuses on the social aspects related to the roles that one occupies in society and finally the interdependence so that is related to emotional fitness as well as to holders of systems, receptive behavior and contribution of behavior identified the patterns of human value, affection, love and affirmation. 2-4 The nursing process should not be seized or held for a mere fulfillment of tasks, as this
- 9. methodological tool scientifically underpins the profession knowledge, allows to develop effective assistance focused on patient safety and provides the identification of individual and collective needs under a holistic and critical view. 5-6 The nursing process comprises phases which vary according to nursing theory adopted. The elements of Roy nursing process include: research behavior, research stimuli, nursing diagnosis, goal setting, intervention and evaluation. The first element consists of collecting answers or the person's behavior in relation to each of the adaptive modes. The second involves the identification of focal, contextual and residual stimuli that are influencing behaviors. The third element of
- 10. the process is the identification of nursing diagnoses, which reflects the nurse's judgment on the level of adaptation of the person. 4, 7 The fourth element includes goal setting, time the nurse lists the resulting behaviors of nursing care. The fifth is for the planning of interventions that should be selected according to pre-established goals, aiming to promote adaptation by stimulating change. Finally, evaluation, it is believed that the effectiveness of nursing intervention is related to human behavior adaptation. 4,7 By analysis of Callista Roy adaptation nursing theory, sees it a theoretical framework for the development of care for people with chronic diseases which need to go
- 11. through a process of adaptation to the new conditions of health and disease, among these the affected by stroke, as this condition creates stimuli that the patient requires an adaptive response. Given the above, the objective of this study is to reporting the experience of the application of the nursing process implemented in the light of the Theory of Adaptation of Callista Roy to a patient affected by stroke. This is a descriptive study of type experience report, resulting from the application of the nursing process mediated by the Nursing Theory of Adaptation of Callista Roy to a hospitalized patient in June, 2013, in a neurological clinic of an emergency hospital
- 12. in the city of Teresina, Piaui. To implement the first phase of the nursing process there was drawn up an interview script with the intention of guiding the research and behavioral stimuli (Appendix A). After behavioral and stimulation research nursing diagnoses were established, using as basis the taxonomy of the North American Nursing Diagnosis Association International (NANDA-I).8 The process of preparing and inference of nursing diagnoses followed the steps recommended by the reasoning of METHOD INTRODUCTION Costa CPV da, Luz MHBA, Bezerra AKF, Rocha SS da. Application of the nursing theory of Callista Roy... English/Portuguese J Nurs UFPE on line., Recife, 10(Suppl. 1):352-60, Jan., 2016
- 13. 354 ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.7901- 80479-1-SP.1001sup201622 Risner, namely: categorization of data, identification of data gaps, clusters of relevant data, comparison between the groups with normal patterns, inferences and propositions of etiological relations. 9 Then it set up goals and interventions needed to promote better adaptive response. The nursing interventions were defined according to the Nursing Interventions Classification (NIC) 10 and are shown in Table 1 with its specific code for each intervention with four digits. For the results we used the taxonomy Nursing Outcomes Classification
- 14. (NOC) 11 identifying the result with their respective specific code, and finally there was the evaluation of the implemented actions. The application of the Roy Adaptation Model allowed identify commitment in the following components of the physiological mode: oxygenation, protection, nutrition, activity and rest, senses and neurological function. In the oxygen component it showed up the following nursing diagnoses according to NANDA-I: ineffective breathing pattern manifested by tachypnea defining characteristics and dyspnea, ineffective airway clearance manifested by ineffective cough, tachypnea, and dyspnea and risk of
- 15. ineffective cardiac tissue perfusion. For the diagnosis of ineffective breathing pattern nursing interventions were: respiratory monitoring, monitoring of vital signs and respiratory control with the following activities: monitoring frequency, pace, depth and effort of breaths, listen breath sounds, monitor diaphragmatic muscle fatigue, monitor and record temperature, pulse, blood pressure and breathing pattern. Interventions facing the diagnosis of ineffective airway clearance were: listen breath sounds, vacuum when necessary, place the patient in order to maximize breathing, encourage slow, deep breathing and guide and encourage the patient to cough after inhaling and exhaling deeply. For the diagnosis of cardiac tissue perfusion ineffective risk
- 16. interventions were listen heart sounds and administering antihypertensive medication, according to prescription. As adaptive problems of the protection component, there are the nursing diagnoses, namely: impaired tissue integrity, impaired skin integrity, which were listed by the patient develops pressure ulcers (UPP) Grade III sacral area and UPP grade II calcaneus region and the diagnosis of impaired oral mucosa, and infection risk. Interventions for the care of UPP were to describe the ulcer features, monitor the color, temperature, edema moisture and appearance of the skin around, monitor wound infection signs, perform changing positions of 2 in 2 hours, advise mattress use appropriate, guide staff and conduct healing
- 17. of the wound. The activities for the intervention of oral health maintenance guide were doing oral hygiene after meals and whenever necessary and guide brush of their teeth, gums and tongue. For the restoration of intervention of oral health activities consisted of guiding the use of brush with soft bristles and monitor lesions on the lips and mucous membranes. For the diagnosis of infection risk interventions were: monitor site of venipuncture, exchange peripheral access where necessary and monitor systemic signs and symptoms and infection sites. In the nutrition component there was detected the nursing diagnosis of impaired dentition related to ineffective oral hygiene evidenced by loss of teeth and halitosis.
- 18. Interventions for these diagnoses were the same as diagnosis of impaired oral mucosa. The physical mobility nursing diagnoses related to impaired neuromuscular impairment evidenced by hemiplegia and disturbed sleep pattern related to environmental changes evidenced by reports of trouble sleeping and staying asleep were listed as adaptive problems of the physiological mode on their activity component and rest. Nursing interventions prescribed for the diagnosis of impaired physical mobility were neurological positioning and therapy exercises with the following activities: avoid applying pressure on the affected side of the body, supporting the affected body part, hold stimuli and passive exercises on the affected
- 19. side, guide family to monitor the realization of exercise and physical therapy forward. For intervention improves sleep has prescribed the following activities: monitor sleep patterns and the amount of hours slept, discouraging daytime sleep and provide comfort measures while sleeping. As the adaptive problem senses component found that the impaired verbal communication and diagnostics risk of falls. The activities for communication improvement intervention were listening, encouraging the patient to repeat words, offer positive reinforcement and support, when necessary, to maintain dialogue with the patient, encourage the patient to talk slowly and observe nonverbal clues. For diagnosing EXPERIENCE REPORTS
- 20. Costa CPV da, Luz MHBA, Bezerra AKF, Rocha SS da. Application of the nursing theory of Callista Roy... English/Portuguese J Nurs UFPE on line., Recife, 10(Suppl. 1):352-60, Jan., 2016 355 ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.7901- 80479-1-SP.1001sup201622 risk of falls, interventions were guiding on the use of assistive devices and guide the patient to call help when jogging. The last mode of the physiological adaptive problem was identified in neurological function component with the nursing diagnosis risk of inefficient brain tissue perfusion. Although the patient be affected by a condition in the neurological system, found only a nursing diagnosis in the component neurological function, this fact can be explained because the neurological function is
- 21. configured as a component of the hardest physiological mode analysis due to the condition of relationship between this complex process and the other components of the physiological mode. 3 Interventions for diagnosis of neurological function component were: monitor the size, shape, symmetry and reactivity of pupils, monitor level of awareness and guidance, applying the Glasgow coma scale, observe headache complaints, monitor speaks characteristics and monitor the presence of signs and symptoms of increased intracranial pressure. In so self-evident that the adaptive problem in self-staff component formed by anxiety as nursing diagnosis. The interventions
- 22. were outlined using a calm and safe approach, explain the procedures to be performed and encourage the patient to verbalize feelings. The last way in which it showed an adaptive problem was the role of performance mode which nursing diagnosis raised was ineffective control of the therapeutic regimen. The activities for the nutrition counseling intervention were to identify the behaviors to be changed, provide information to diet modification and discuss preferences and food which the patient does not like. For behavior modification intervention activities were encouraging the replacement of undesirable habits by desirable habits, discussing the process of change with the patient and caregiver and promote family involvement in the change process.
- 23. The last step of the nursing process, as Callista Roy, is the evaluation in which the nurse questions and weaves judgment about the achievement of objectives in the process of adaptation by which the individual passes. After 3 days of use of the nursing process based on Roy's theory in patient care it will found that interventions have allowed changes in decreased anxiety with positive patient discourse and planning for execution of daily life activities after hospital discharge configurating itself change in strategy planning indicator is inserted into the nursing outcome "self-anxiety." To the result of level of anxiety became evident change in the indicator improved in the pattern of sleep and rest of patients with nocturnal sleep improvement report allowing adaptation of
- 24. the patient to self-concept mode and activity and rest. The physiological mode results achieved for the diagnosis of oral hygiene with an improvement in halitosis indicator and the inefficient respiratory pattern diagnosis and ineffective airway clearance with changes in respiratory rate indicators and dyspnea at rest and the result of vital signs there was change in respiratory rate indicator. The mode of performance was a result of knowledge and control of hypertension with changes in control benefits indicators of the disease and strategies to improve adherence to diet and result of family support during treatment with change in the collaboration window with family sick in determining the care and information request indicator.
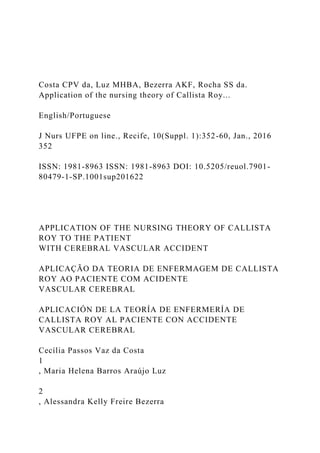
- 25. The other results listed in Figure 1 represent the expected results compared to the listed diagnoses and nursing interventions. Costa CPV da, Luz MHBA, Bezerra AKF, Rocha SS da. Application of the nursing theory of Callista Roy... English/Portuguese J Nurs UFPE on line., Recife, 10(Suppl. 1):352-60, Jan., 2016 356 ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.7901- 80479-1-SP.1001sup201622 Component Mode of Adaptation Nursing diagnosis (NANDA-I) Nursing intervention (NIC)-Code of NIC Nursing results (NOC)
- 26. Physiological Oxygenation Ineffective breathing pattern related to hyperventilation manifested by tachypnea and dyspnea Respiratory monitoring (3350). Monitoring of vital signs (6680). Airway control (3140). Respiratory status (0415). Vital signs (0802). Oxygenation Ineffective airway clearance related to neuromuscular dysfunction and smoking shown by ineffective cough, tachypnea and dyspnea. Respiratory monitoring (3350). Airway control (3140). Stimulus to cough (3250) Respiratory status: airway permeability (0410). Respiratory status: ventilation (0403).
- 27. Oxygenation Risk of cardiac tissue perfusion related to decreased hypertension and hyperlipidemia. Monitoring of vital signs (6680). Tissue: cardiac perfusion (0405). Vital signs (0802). Protection Impaired tissue integrity related to impaired mobility, decreased dermal vascularization secondary to ageing and moisture evidenced by grade III pressure ulcer on sacral region. Caring for pressure ulcers (3520). Wound healing: second intention (1103). Tissue integrity: skin and mucous membranes (1101). Physiological
- 28. Protection Impaired skin integrity related to motor deficit, impaired mobility and decreased Vascularity secondary dermal aging evidenced by grade II pressure ulcer in calcaneal region. Caring for pressure ulcers (3520). Wound healing: second intention (1103). Tissue integrity: skin and mucous membranes (1101). Protection The oral mucosa impaired related to ineffective oral hygiene evidenced by tongue coated, oral lesion and halitosis. Maintenance of oral health (1710). Restoration of oral health (1730) Oral hygiene (1100). Protection Risk of infection related to invasive procedures. Protection against infection (6550) Risk control: infectious process (1924). Nutrition Impaired dentition related to ineffective oral hygiene evidenced by loss of teeth and halitosis. Maintenance of oral health (1710). Restoration of oral health (1730). Oral hygiene (1100).
- 29. Activity and rest Impaired physical mobility related to neuromuscular impairment evidenced by hemiplegia. Neurological positioning (0844). Exercise therapy: joint mobility (0224). Body mechanics performance (1616). Mobility (0208). Physiological Activity and rest Disturbed sleep pattern related to environmental changes, evidenced by reports of difficulty to sleep and stay asleep. Sleep improvement (1850). Sleep (0004). Senses Impaired verbal communication related to changes in the
- 30. central nervous system, manifested by dysarthria. Improvement of communication: speech deficit (4976). Listen actively (4920). Communication (0902). Communication: expression (0903). Senses Risk of falls related to impaired physical mobility. Prevention of falls (6490). Risk control (1902). Care with the affected side (0918). Neurological Function Risk of cerebral tissue perfusion ineffective related to cerebral aneurysm and hypertension. Neurological monitoring (2620). Monitoring of vital signs (6680). Tissue perfusion: cerebral (0406). Neurological State (0909). Self-concept Self-personal Disease-related anxiety manifested by crying and insomnia. Anxiety reduction (5820). Level of anxiety (1211). Anxiety self-control (1402). Role performance Ineffective therapeutic regimen related control the
- 31. complexity of the treatment regimen indicated for failure to take action to reduce risk factors. Nutritional counseling (5246). Behavior modification (4360). Knowledge: control of hypertension (1837). Family support during treatment (2609). Figure 1. Diagnoses, interventions and outcomes of nursing for a patient with STROKE according to the Adaptive Model of Roy. Teresina-PI, 2014. Santos FS, Arruda AJCG de, Vasconcelos JMB. Aplicabilidade do código de ética nas ações... English/Portuguese J Nurs UFPE on line., Recife, 10(Suppl. 1):352-60, Jan., 2016 357 ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.8423- 73529-1-RV1001201601 The grounded nursing process in Roy's theory contributed to effective nursing care to patients affected by stroke to give importance to the stimuli that trigger responses which require the adaptation of the patient.
- 32. Before long the patient has demonstrated adaptive behaviors with regard to diagnosis of oral hygiene, ineffective breathing pattern, and ineffective airway pattern of sleep and rest, anxiety and ineffective control of the therapeutic regimen. In view of this is salutary that care implemented resulting from the nursing process based on the theoretical model of Roy and the use of NANDA-I taxonomy, NIC and NOC allowed direct the activities to adaptive problems contributing to the adaptation of the patient, and provide scientific nature to care practice with consequent empowering care by nurses. Therefore, the experience raises the need to use a conceptual framework in nursing care.
- 33. 1. Organização Mundial de Saúde. Cuidados inovadores para condições crônicas: componentes estruturais de ação. Relatório mundial. Organização Mundial da Saúde. Brasília, 2003 [Internet]. [cited 2013 July 5]. Available from: http://www.who.int/chp/knowledge/publicat ions/icccportuguese.pdf 2. Roy C, Andrews HA. The Roy adaptation model. Stamford: Appleton e Lange; 1999. 3. Lopes MVO, Araújo TL, Rodrigues DP. A relação entre os modos adaptativos de ROY e a taxonomia de diagnósticos de enfermagem da NANDA. Rev Latino-Am Enfermagem [Internet]. 1999; [cited 2013 July 12];7(4):97- 104. Available from: http://www.scielo.br/scielo.php?script=sci_ar ttext&pid=S0104-
- 34. 11691999000400013&lng=en&nrm=iso 4. George JB. Teorias de enfermagem: os fundamentos à prática profissional. Porto Alegre: Artes Médicas; 2000. 5. Pereira CFD, Tourinho FSV, Miranda FAN, Medeiros SM. Ensino do processo de enfermagem: análise contextual. J Nurs UFPE on line [Internet]. 2014 [cited 2014 Mar 15];8(3):757-64. Available from: http://www.revista.ufpe.br/revistaenfermage m/index.php/revista/article/view/5473 6. Freitas NF, Tannure MC, Chianca TCM. Implementation of nursing process in a neonatal intensive care unit of Belo Horizonte. J Nurs UFPE on line [Internet]. 2010 [cited 2014 Jan 10];4(esp):1287-293. Available from: http://www.revista.ufpe.br/revistaenfermage
- 35. m/index.php/revista/article/view/1053/pdf_ 94 7. Coelho SMS, Mendes IMDM. Da pesquisa à prática de enfermagem aplicando o modelo de adaptação de Roy. Esc Anna Nery [Internet]. 2011 Dec [cited 2013 July 11];15(4):845-50. Available from: http://www.scielo.br/scielo.php?script=sci_ar ttext&pid=S1414- 81452011000400026&lng=en&nrm=iso 8. North American Nursing Diagnosis Association International (NANDA-I). Diagnóstico de enfermagem da NANDA: definições e classificação - 2012-2014. Porto Alegre: Artmed; 2013. 9. Risner PB. Diagnosis: analysis and synthesis of data. In: Griffith-Kenney JW, Christensen PJ. Nursing Process application of
- 36. theories, frameworks, and models. 2nd ed. St. Louis Mosby; 1986 10. Buthcher H, Bulechek GM. Classificação das Intervenções de Enfermagem (NIC). 3 ed. Porto Alegre: Artmed; 2004. 11. Moorhead S, Johnson M, Maas M. Classificação dos resultados de enfermagem (NOC). 4th ed. Rio de Janeiro: Elsevier; 2010.
- 38. Aplicabilidade do código de ética nas ações... English/Portuguese J Nurs UFPE on line., Recife, 10(Suppl. 1):352-60, Jan., 2016 358 ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.8423- 73529-1-RV1001201601 GUIDE FOR BEHAVIORAL AND STIMULUS RESEARCH Name: ___________________________________________________ Birthdate: ________________ Age: _____________________ Gender: ( ) Male ( ) Female Skin color: ( ) White ( ) Black ( ) Yellow ( ) Maroon Marital status: ( ) Married ( ) Single ( ) Widower/Widow ( ) Separated ( ) Stable union Schooling: ( ) Illiterate ( ) Incomplete elementary school ( ) Complete elementary school ( ) Incomplete high school ( ) Complete high school ( )
- 39. Incomplete higher education ( ) Complete higher education Occupation: _____________________________________________________ _ Address: _____________________________________________________ __ City: ________________________ State: _________________________ Date of admission: ___________________ Origin: Home Hospital Other: ________________ Nursing: ________________ Bed: _________________ 2 PHYSIOLOGICAL MODES 2.1 OXIGENATION 2.1.1 Breath Breath: ( ) Spontaneous ( ) Nasal catheter ( ) Mask Chest: ( ) Flat ( ) Cask or Barrel ( ) Funnel-shaped ( ) Carinate
- 40. Other: ___________________________ Respiratory frequency: __________ respiratory movements per minute Respiratory auscultation: ( ) Adventitious noise absent ( ) Adventitious noises present: ( ) Snoring ( ) Ping ( ) Rattle Other: _________ Cough: ( ) No ( ) Yes: ( ) Nonproductive ( ) Productive 2.2.2 Circulation Blood pressure: ___________mmHg Heart frequency: ______bpm Pulse: ( ) Regular ( ) Irregular ( ) Thready ( ) Full ( ) Impalpable Capillary filling time: ________seconds The presence of edema: ( ) No ( ) Yes: ( ) MMSS ( ) MMII Other: ____________ 2.2 NUTRITION AND ELIMINATION Diet: ( ) Oral ( ) SNG ( ) SNE ( ) Parenteral Dentition: ( ) Absence of teeth ( ) Loss of teeth ( )
- 41. Presence of teeth Oral mucosa: ( ) Full ( ) With lesions Oral hygiene: ( ) Unsatisfactory ( ) Satisfactory Abdomen: ( ) Flat ( ) Globulous ( ) Distended ( ) Flaccid ( ) Painful on palpation Fluid intake per day: ( ) less than 5 glasses ( ) 5-10 glasses ( ) more than 10 glasses Number of meals a day: ( ) less than 3 meals ( ) between 3- 5 meals ( ) more than 5 meals Weight: ______kg Height: _____m BMI: _________ Bowel sounds: ( ) Absent ( ) Present ( ) Increased ( ) Diminished Nausea: ( ) No ( ) Yes Vomiting: ( ) No ( ) Yes Dyspepsia: ( ) No ( ) Yes Diarrhea: ( ) No ( ) Yes Frequency of defecation: __________times per week APPENDIX
- 42. Santos FS, Arruda AJCG de, Vasconcelos JMB. Aplicabilidade do código de ética nas ações... English/Portuguese J Nurs UFPE on line., Recife, 10(Suppl. 1):352-60, Jan., 2016 359 ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.8423- 73529-1-RV1001201601 Date of the last defecation: _______________ Urinary elimination: ( ) Spontaneous ( ) SVD ( ) Urinary device ( ) Urinary retention ( ) Urinary incontinence ( ) Dysuria ( ) Hematuria ( ) Anuria ( ) Oliguria Urinary volume: __________ 2.3 Activity/rest and protection, and four complex processes (sensitive, liquid and electrolytes, neurological function and endocrine function). Sleep: ( ) Increased ( ) Diminished ( ) Without complaints Sleep on the day shift: ( ) No ( ) Yes: _________hours Mobility: ( ) Not changed ( ) Changed: __________________________ Mucous membranes: ( ) Normochromic ( ) Hypochromic _____/4+ ( ) Icteric
- 43. Eyes: ( ) Jaundice ( ) Eyelid edema Other: ______________ Skin: ( ) Normal ( ) Cyanosis ( ) Jaundice ( ) Pallor Wound: ( ) No ( ) Yes Local: ________________________________ Dimensions: _____________________________________________________ _ CLASSIFICATION: The wound: ( ) Closed ( ) Open ( ) Chronic ( ) Acute The tissue: ( ) Necrosis ( ) Mortification of tissues ( ) Granulation ( ) Epithelialization The exudate: ( ) Serous ( ) Sanguineous ( ) Purulent ( ) Fibrinous exudation Quantity of the exudate: ( ) Small ( ) Moderate ( ) Intense ( ) Abundant Odor: ( ) Odorless ( ) Fetid Recommended therapy for wound treatment: _____________________________________________________ __________
- 44. 2.4 NEUROLOGICAL FUNCTION Glasgow Coma Scale: Eye Opening: ______ Verbal answer: __________ Motor answer: ________ Pupils: ( ) Equal ( ) Anisocoric ( ) Miosis on the right ( ) Miosis on the left ( ) Mydriasis on the right ( ) Mydriasis on the left Conscious: ( ) Yes ( ) No Guided: ( ) Yes ( ) No 3. What do you know about your present illness? _____________________________________________________ __________ 4. Important complaints: _____________________________________________________ _________________________________ _____________________________________________________ _________________________________ _________________ VITAL SIGNS:
- 45. T: _______ P: _________ R: _________ PA: _______ IMPORTANT LABORATORY DATA: _____________________________________________________ _________________________________ _____________________________________________________ _________________________________ ________________ ________________________________________________ SIGNATURE Santos FS, Arruda AJCG de, Vasconcelos JMB. Aplicabilidade do código de ética nas ações... English/Portuguese J Nurs UFPE on line., Recife, 10(Suppl. 1):352-60, Jan., 2016 360 ISSN: 1981-8963 ISSN: 1981-8963 DOI: 10.5205/reuol.8423- 73529-1-RV1001201601 Submission: 04/07/2015 Accepted: 25/07/2015
- 46. Published: 01/01/2016 Correspondence Address Cecília Passos Vaz da Costa Avenida Centenário, 3052 Bairro Aeroporto CEP 64003- Copyright of Journal of Nursing UFPE / Revista de Enfermagem UFPE is the property of Revista de Enfermagem UFPE and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use. Running head: ACA 1 ACA 10 Changes resulting from the Affordable Health Care for America Act (ACA) Weltee Wolo Rasmussen College
- 47. Author Note This paper is being submitted on May 28, 2017, Kristi Downs’s Healthcare Planning and Policy Management H360/HSA4150 course The Affordable health care act was a series of changes and reforms that were directed towards the health sector. The bill got signed into law in March 2010. The reforms aimed at improving the quality of health care for the American population (Protection & Act, 2010). They are a set of rules for health care facilities, insurance companies and other businesses on matters to do with the provision of health care to people. Much as there are changes the overall perception is that there has had a tremendously positive effect on the people of America as they can now comfortably rely on the act to have their medical issues taken care of without worrying too much about paying. According to Huntington et al. (2011), the bill has substantially made health care affordable and attainable by most of the people in the US. Ever since it’s passing the bill has had tremendous changes in some primary health care providers such as insurance companies, health care providers, and the facilities. The changes range from those that are negative and those that are positive, from the long term to the short term goals. One of the providers that have been affected the most by the law is the insurance companies and the way that they operate. Possible causes of change to the insurance unit The changes have had to take place so as to accommodate the titles of the ACA of 2010. The biggest and most recognizable cause of the changes is the fact that the law calls for the increase in the number of people who get health care in the country. More people of all classes and social standing automatically request the adjustment of operation and systems
- 48. within insurance companies (Cantor et al., 2012). There is the need to reduce the amount of money being spent by individuals in health care without having to compromise the quality of care. What this implies is that companies and businesses that take care of issues of insurance substantially need to check their systems so as to be viable and up to the task of meeting the needs of the people and fulfilling the law of ACA. According to Blumenthal & Collins (2014), most of these changes are not temporary as they are static unless there is a reversal of the law they are for the long term. Naturally, the insurance companies are the ones that are most affected by the act. This is because most of the components of the law deal with issues of money as well as health care quality. As a result of this, it is critical that the effects of the changes be evaluated by what takes on a temporary standing and those that are for the long term. The short term effects are those that are quickly forgotten based on the minimal impact that they have. On the other hand, the long-term effects are more permanent and affect the company the greatest. Effects of the Affordable Care Act on insurance companies Education of consumers – more power to consumers The ACA is one document that has brought about enlightenment to the consumer when it comes to matters of health care. People can conveniently take control of their lives and what facilities that they would want to have the care in (Huntington et al., 2011). With more private insurance firms coming up to fill the gap which is used to fulfill the needs of the people, there is the emergence of the need to conduct consumer education. Berwick & Hackbarth (2012), state that consumer education ensures that people make choices that are informed and with adequate knowledge on the issue. There is a possibility that people could under buy or over buy the policies and harm them financially in the long run. The ACA has mandated the insurance companies to offer very valid and more information on their policies and has even made it simpler for more understanding. In the beginning, these companies would quickly hide facts and
- 49. figures in very complicated insurance terminology that was not understandable upfront. This could easily mislead people into buying things that they did not understand or be deceived into buying policies that did not meet their needs entirely (Blumenthal & Collins, 2014). Deception and poor understanding are a thing of the past according to the new act. People now have a choice among many options, and they do so after accessing the relevant information. Accommodation of more people Some of the ways through which insurance companies accommodate more people is by increasing the coverage limits, mandating private business owners with fifty additional employees to offer medical insurance to its employees, not using medical conditions to provide medical cover and stopping the idea of people losing protection based on the seriousness of their diseases (Rosenbaum, 2011). All these are strategies employed by the ACA to increase the number of people being covered by the medical health plans under the act. For the insurance companies, this translates once again to fiscal adjustments. As of 2009, there were fewer businesses that could not facilitate accommodation for every individual that needed to be covered. For instance, with this act, there has been accommodation of younger people as compared to previous years where older people were included (Cantor et al., 2012). Insurance companies have had to establish safeguards so as to ensure that the premiums offered were enough to cover the extra costs that would accommodate all the additional people that have had to be covered. Safeguards are meant to reduce consumer spending, increase insurance companies spending and eventually ensure that costs of all the medical care for individuals that deserve and have covered are catered to properly. Financial The ACA has significant financial implication for the insurance companies all around the state. The cat called for the coverage
- 50. of people and therefore more planning and the need to establish more sources of funds emerged. The private firms also saw a chance to get a place in the market. The act also increases the amount of money that the government allocates for the companies. Much as the government assists the companies in their funding, the amount used to cover the cost official care is far more than they can get from the government. Retaining a for-profit healthcare system has economic benefits this mostly applies to the private insurance companies who are set to cater to the needs of the people as well as make profits to remain in the market and relevant (Sommers et al., 2015). This also means that the system’s aspects also need to gain benefit so as to stay relevant. While the ACA aims at reducing the cost of health care Americans are still among the people paying the most for basic health care. These are some of the adjustments that companies have to take care of. The other financial implication of the Affordable Care Act is that of reduction of annual revenue of insurance companies. According to Blumenthal & Collins (2014), while the insurers had to make adjustments to suit the demands of the ACA, the clients to these insurers were not affected as they were not expected to make adjusted contributions to also adjust to the ACA marketplace. This had them making assumed projection, and these assumptions did not work as projected since this was a first time experience. The result of this was that insurers did worse in their performance unlike in previous years. Many of the insurers underestimated the claims by over thirty-five percent for the high claimants. On the other hand, the lower providers underestimated their own by over four percent. Both of these were equivalent to a six percent deviation from the global market share of claims. In the preceding years, there have been evidence of more accurate projections, but the losses have been permanent as most of the newer and smaller insurers have had difficulty in gaining their financial round with many of them closing shop due to bankruptcy.
- 51. Competition in business – insurance market place The ACA makes room for the establishment of an insurance marketplace. This is where people get to make informed choices based on the type of insurance that they want and the amount of money available (Berwick & Hackbarth, 2012). Unlike in the past, the insurance companies have been mandated with the duty of making known and transparent all the information about it as much as possible so as to facilitate in decision making. As a result of this companies may have to make adjustments to their services and premiums so as to attract more clients to its companies. The competition for customers increases and this calls for the need for changes. According to Protection & Act (2010), many insurance companies have had to take on extreme measures so as to attract more customers. Those with difficulty in adjusting may have had to take adverse measures such that they have run out of business. Lack of clients or their reduction in number equally results into the making of losses for the company. This means that these companies have had to run out of business and close shop. Business is threatened by the need to adjust premiums and rates. People have the power to choose the policies and companies that they feel serve their needs without feeling oppressed by them. The failure to comply with the policies of the Act will bring about the tight competition that makes the other companies better their offers so as to attract more clients. Competition in this business has had extreme effects that work to the advantage of the patients by regulation of costs and quality (Rosenbaum, 2011). Medical conditions covered – preexisting conditions With the signing in of the ACA, insurance companies have had to change the type of conditions that they cover. Before the law was implemented, people were limited to insurance cover based on their present health conditions. There was an increased chance that people with chronic illnesses before their application would be left out of coverage based on these
- 52. circumstances. With the inception of the Affordable health care act into law, insurance companies have had formulated policies that accommodate children and adults even if they had preexisting conditions that initially barred them from getting covered (Rosenbaum, 2011). This was a measure that the insurers made the most of their revenue by reducing associated risks which were to be borne by the individual as opposed to the company. For this reason, the insurer has had to deal with extra costs incurred by the people who are suffering from chronic diseases other conditions that may have had to be addressed at a cheaper cost. Due to the fact that a person only pays a limited amount of money for their cover, the insurance company is the one that cushions the extra fees. In addition to the medical conditions covered insurance companies have had to deal with the limitation of the conditions that could lead to one losing their cover. These have been reduced to accommodate those people who may have made an honest mistake while making their application or may have developed a complication that was beyond their control or previous awareness (Sommers et al., 2015). Initially, insurance companies had the power to dismiss a cover for mistakes made and complications developed even after providing the person with medical cover. This implies that once again the insurer has to part with more money to provide essential services without charging the client more to get the same services. Increase in coverage limit The act has changed the age limit for coverage. It is flexible enough, and the insurance policies have been mandated with the task of covering children under their parents for up to twenty- six years of age. These have deep fiscal implications that have the long-term impact on the companies. These have further long-term financial consequences to these enterprises. There is a need for flexibility, and without proper planning, most of these businesses may quickly run out of business based on the
- 53. fact that they are not financially prepared for these changes. As of 2016 many of the newly established insurers have had to go into financial distress to the extent of failing and going out of business. The effect has also been seen in the larger companies such as United Healthcare which have so far withdrawn from the ACA’s exchange market due to the important financial losses that it had been facing. The insurers as of 2016 only managed to make only two percent of profits higher than the projected profits in 2010 even after the account reinsurance payment done. This is evidence of the deep financial plunges that insurance companies have had to deal with as a result of actions such as increasing the insurance cover limit. In conclusion, the new health care act has had a very great impact on the insurance companies. This range from fiscal implications to having to accommodate more people at a smaller cost than it was before. Many adjustments have therefore been made to accommodate these changes. The greatest impact of all time is that these companies have shifted focus from making more money from claims to ensuring that everybody gets an insurance policy or treated at a lower cost. These companies have often focused on making money for themselves at times compromising the health of the patients. These include situations such as dropping of patients due to complications developed so as to cut the costs of money discharged by the insurance companies. Much as there seem to be more negative impacts as opposed to the positive ones, the insurance companies may have ultimately been favored as they have more people to cover thereby accumulating more money while offering better services to the people. Finally, the ACA has enabled more companies to crop into the market thus creating equilibrium as more money has been allocated by the federal government to support the provision of better health care for people. References Berwick, D. M., & Hackbarth, A. D. (2012). Eliminating waste in US health
- 54. care. Jama, 307(14), 1513-1516. Blumenthal, D., & Collins, S. R. (2014). Health care coverage under the Affordable Care Act—a progress report. Cantor, J. C., Monheit, A. C., DeLia, D., & Lloyd, K. (2012). Early impact of the Affordable Care Act on health insurance coverage of young adults. Health services research, 47(5), 1773-1790. Protection, P., & Act, A. C. (2010). Patient protection and affordable care act. Pu Huntington, W. V., Covington, L. A., Center, P. P., Covington, L. A., & Manchikanti, L. (2011). Patient Protection and Affordable Care Act of 2010: reforming the health care reform for the new decade. Pain Physician, 14(1), E35-E67.blic Law, 111, 48. Rosenbaum, S. (2011). The Patient Protection and Affordable Care Act: implications for public health policy and practice. Public health reports, 126(1), 130- 135. Sommers, B. D., Gunja, M. Z., Finegold, K., & Musco, T. (2015). Changes in self-reported insurance coverage, access to care, and health under the Affordable Care Act. Jama, 314(4), 366-374. HEALTH CARE PROVIDER 1
- 55. Health care provider Weltee Wolo Rasmussen College Author Note This paper is being submitted on April 20, 2017, Kristi Downs’s Healthcare Planning and Policy Management H360/HSA4150 course Health care provider Health care provider is a term that is used to describe a business or an individual who is authorized by the state to perform to consumer’s health care services. An example of such a health care provider is a doctor office. It is considered as medical premises where one or more patients are provided with treatment by one or more doctors. With the implementation of the health care act, it was noted that time spent between physicians and patients reduced. This was due to the mounting duties that are non-clinical and reimbursement decline, thus leading to minimal patient-doctor contact. With this, it means the patient would not have a consistent follow-up care due to the use of patient extenders by doctors in office (U.S. Department of Health & Human Services, n.d).
- 56. References U.S. Department of Health & Human Services. (n.d). About Affordable Care. Retrieved from https://www.healthcare.gov/get-coverage/ HEALTH CARE PROVIDER 3 Health care provider Weltee Wolo Rasmussen College Author Note This paper is being submitted on April 20, 2017, Kristi Downs’s Healthcare Planning and Policy Management H360/HSA4150 course Health care provider A hospital is an example of a health care provider. It is responsible for the provision of short-term care to individuals with serious health issues which might be an outcome of a disease, injury or abnormality. With the implementation of the health care act, the hospital was one place that was affected. It is considered that most of these impacts were positive. There was an increase of the community fund. Which provided recognized health centers the right to provide medical services to populations that are considered underserved and are often shut down from departments of emergency. With the health act
- 57. in place, there was a reduction of uncompensated care in hospitals. That meant there was an improvement of access to coverage care of patients due to the creation of patient and state stability fund. There is the restoration of DHS which hospitals stand to benefit from (American Hospital Association, 2016). It is also considered that all is not well since, with the legislation on the proposal, the levels of insured would reduce. And in the process, no Medicare rates would be restored to the higher levels of ACA-level. Also, there is the issue of greater flexibility concerning requirements of coverage, which has implications for hospitals (American Hospital Association, 2016). References American Hospital Association. (2016). Hospitals are economic anchors of community. Retrieved from http://www.aha.org. Running head: HEALTH CARE PROVIDERS 1 HEALTH CARE PROVIDERS 3 Annotated bibliography for health care providers Weltee Wolo Rasmussen College Author Note This paper is being submitted on May 07, 2017, Kristi Downs’s
- 58. Healthcare Planning and Policy Management H360/HSA4150 course Eichenwald, S., Petterson, B. J., & Wapola, J. (2014). Using the electronic health record in the health care provider practice. Clifton Park, NY: Delmar. This book is a practical guide that discusses all the aspects of electronic health record (EHR) at health facilities. The book addresses the various types and functions of EHR use namely administrative functioning EHRs and Clinical functioning EHRs. This book is a resourceful tool for the purpose of understanding just what the categories of EHRs are and how they apply to the healthcare facilities. It further emphasizes the fact that EHR is an essential part of modern health care operation today. This book will contribute to my project as it highlights the various aspects of EHR and I will utilize this information to conclude the relevance of modernity in the health care organization. In Shirazian, T., & In Gertz, E. (2013). Around the Globe for Women's Health: A Practical Guide for the Health Care Provider. The book gives an in-depth account of the value of culture by communication and cultural knowledge for health care providers dealing with women's health. This is a basic need when it comes to this century's type of care which targets equity, sensibility and improved care for health care for the women. There are specific chapters that touch on the specific health conditions that mainly affect the women population. This is a resourceful book as it gives insight to health provision for this particular health population. I will use this book as a source for my project as it has information that contributes positively to my project. Health care is all rounded and focuses on a different population. For this specific project, I will highlight on the
- 59. women population. U.S. Department of Health & Human Services. (n.d). About Affordable Care. Retrieved from https://www.healthcare.gov/get-coverage/ Medical health insurance cover is a very important thing to have in these times. This is the best way through which an individual can have their medication paid for. It is paperless form of payment. This website gives a variety of options that individuals can use to pay for the medical care including which conditions necessitate the use of insurance such as having a new baby and cushioning expensive emergency procedures. The government website is the ultimate compilation of justifications and workable data thus the information provided is highly reliable. I will use this information from this website to justify the use and advantages of adopting health insurance among households at health care facilities. American Hospital Association. (2016). Hospitals are economic anchors of community. Retrieved from http://www.aha.org. This website is a critical one as it gives detailed information on the uses and application of health care facilities in America. These vary from the type of hospitals in America to the specific type of resources that they deal with. Once again the information in this website facilitates the understanding of the role of a hospital in a community. In my project this will facilitate in the distinction between the different types of facilities and the role that they play in the community as well. Running head: ACA 1 ACA 10 Changes resulting from the Affordable Health Care for America Act (ACA)
- 60. Weltee Wolo Rasmussen College Author Note This paper is being submitted on May 28, 2017, Kristi Downs’s Healthcare Planning and Policy Management H360/HSA4150 course The Affordable health care act was a series of changes and reforms that were directed towards the health sector. The bill got signed into law in March 2010. The reforms aimed at improving the quality of health care for the American population (Protection & Act, 2010). They are a set of rules for health care facilities, insurance companies and other businesses on matters to do with the provision of health care to people. Much as there are changes the overall perception is that there has had a tremendously positive effect on the people of America as they can now comfortably rely on the act to have their medical issues taken care of without worrying too much about paying. According to Huntington et al. (2011), the bill has substantially made health care affordable and attainable by most of the people in the US. Ever since it’s passing the bill has had tremendous changes in some primary health care providers such as insurance companies, health care providers, and the facilities. The changes range from those that are negative and those that are positive, from the long term to the short term goals. One of the providers that have been affected the most by the law is the insurance companies and the way that they operate. Possible causes of change to the insurance unit The changes have had to take place so as to accommodate the
- 61. titles of the ACA of 2010. The biggest and most recognizable cause of the changes is the fact that the law calls for the increase in the number of people who get health care in the country. More people of all classes and social standing automatically request the adjustment of operation and systems within insurance companies (Cantor et al., 2012). There is the need to reduce the amount of money being spent by individuals in health care without having to compromise the quality of care. What this implies is that companies and businesses that take care of issues of insurance substantially need to check their systems so as to be viable and up to the task of meeting the needs of the people and fulfilling the law of ACA. According to Blumenthal & Collins (2014), most of these changes are not temporary as they are static unless there is a reversal of the law they are for the long term. Naturally, the insurance companies are the ones that are most affected by the act. This is because most of the components of the law deal with issues of money as well as health care quality. As a result of this, it is critical that the effects of the changes be evaluated by what takes on a temporary standing and those that are for the long term. The short term effects are those that are quickly forgotten based on the minimal impact that they have. On the other hand, the long-term effects are more permanent and affect the company the greatest. Effects of the Affordable Care Act on insurance companies Education of consumers – more power to consumers The ACA is one document that has brought about enlightenment to the consumer when it comes to matters of health care. People can conveniently take control of their lives and what facilities that they would want to have the care in (Huntington et al., 2011). With more private insurance firms coming up to fill the gap which is used to fulfill the needs of the people, there is the emergence of the need to conduct consumer education. Berwick & Hackbarth (2012), state that consumer education ensures that people make choices that are informed and with adequate knowledge on the issue. There is a possibility that people could
- 62. under buy or over buy the policies and harm them financially in the long run. The ACA has mandated the insurance companies to offer very valid and more information on their policies and has even made it simpler for more understanding. In the beginning, these companies would quickly hide facts and figures in very complicated insurance terminology that was not understandable upfront. This could easily mislead people into buying things that they did not understand or be deceived into buying policies that did not meet their needs entirely (Blumenthal & Collins, 2014). Deception and poor understanding are a thing of the past according to the new act. People now have a choice among many options, and they do so after accessing the relevant information. Accommodation of more people Some of the ways through which insurance companies accommodate more people is by increasing the coverage limits, mandating private business owners with fifty additional employees to offer medical insurance to its employees, not using medical conditions to provide medical cover and stopping the idea of people losing protection based on the seriousness of their diseases (Rosenbaum, 2011). All these are strategies employed by the ACA to increase the number of people being covered by the medical health plans under the act. For the insurance companies, this translates once again to fiscal adjustments. As of 2009, there were fewer businesses that could not facilitate accommodation for every individual that needed to be covered. For instance, with this act, there has been accommodation of younger people as compared to previous years where older people were included (Cantor et al., 2012). Insurance companies have had to establish safeguards so as to ensure that the premiums offered were enough to cover the extra costs that would accommodate all the additional people that have had to be covered. Safeguards are meant to reduce consumer spending, increase insurance companies spending and eventually ensure
- 63. that costs of all the medical care for individuals that deserve and have covered are catered to properly. Financial The ACA has significant financial implication for the insurance companies all around the state. The cat called for the coverage of people and therefore more planning and the need to establish more sources of funds emerged. The private firms also saw a chance to get a place in the market. The act also increases the amount of money that the government allocates for the companies. Much as the government assists the companies in their funding, the amount used to cover the cost official care is far more than they can get from the government. Retaining a for-profit healthcare system has economic benefits this mostly applies to the private insurance companies who are set to cater to the needs of the people as well as make profits to remain in the market and relevant (Sommers et al., 2015). This also means that the system’s aspects also need to gain benefit so as to stay relevant. While the ACA aims at reducing the cost of health care Americans are still among the people paying the most for basic health care. These are some of the adjustments that companies have to take care of. The other financial implication of the Affordable Care Act is that of reduction of annual revenue of insurance companies. According to Blumenthal & Collins (2014), while the insurers had to make adjustments to suit the demands of the ACA, the clients to these insurers were not affected as they were not expected to make adjusted contributions to also adjust to the ACA marketplace. This had them making assumed projection, and these assumptions did not work as projected since this was a first time experience. The result of this was that insurers did worse in their performance unlike in previous years. Many of the insurers underestimated the claims by over thirty-five percent for the high claimants. On the other hand, the lower providers underestimated their own by over four percent. Both of these were equivalent to a six percent deviation from the
- 64. global market share of claims. In the preceding years, there have been evidence of more accurate projections, but the losses have been permanent as most of the newer and smaller insurers have had difficulty in gaining their financial round with many of them closing shop due to bankruptcy. Competition in business – insurance market place The ACA makes room for the establishment of an insurance marketplace. This is where people get to make informed choices based on the type of insurance that they want and the amount of money available (Berwick & Hackbarth, 2012). Unlike in the past, the insurance companies have been mandated with the duty of making known and transparent all the information about it as much as possible so as to facilitate in decision making. As a result of this companies may have to make adjustments to their services and premiums so as to attract more clients to its companies. The competition for customers increases and this calls for the need for changes. According to Protection & Act (2010), many insurance companies have had to take on extreme measures so as to attract more customers. Those with difficulty in adjusting may have had to take adverse measures such that they have run out of business. Lack of clients or their reduction in number equally results into the making of losses for the company. This means that these companies have had to run out of business and close shop. Business is threatened by the need to adjust premiums and rates. People have the power to choose the policies and companies that they feel serve their needs without feeling oppressed by them. The failure to comply with the policies of the Act will bring about the tight competition that makes the other companies better their offers so as to attract more clients. Competition in this business has had extreme effects that work to the advantage of the patients by regulation of costs and quality (Rosenbaum, 2011). Medical conditions covered – preexisting conditions With the signing in of the ACA, insurance companies have had
- 65. to change the type of conditions that they cover. Before the law was implemented, people were limited to insurance cover based on their present health conditions. There was an increased chance that people with chronic illnesses before their application would be left out of coverage based on these circumstances. With the inception of the Affordable health care act into law, insurance companies have had formulated policies that accommodate children and adults even if they had preexisting conditions that initially barred them from getting covered (Rosenbaum, 2011). This was a measure that the insurers made the most of their revenue by reducing associated risks which were to be borne by the individual as opposed to the company. For this reason, the insurer has had to deal with extra costs incurred by the people who are suffering from chronic diseases other conditions that may have had to be addressed at a cheaper cost. Due to the fact that a person only pays a limited amount of money for their cover, the insurance company is the one that cushions the extra fees. In addition to the medical conditions covered insurance companies have had to deal with the limitation of the conditions that could lead to one losing their cover. These have been reduced to accommodate those people who may have made an honest mistake while making their application or may have developed a complication that was beyond their control or previous awareness (Sommers et al., 2015). Initially, insurance companies had the power to dismiss a cover for mistakes made and complications developed even after providing the person with medical cover. This implies that once again the insurer has to part with more money to provide essential services without charging the client more to get the same services. Increase in coverage limit The act has changed the age limit for coverage. It is flexible enough, and the insurance policies have been mandated with the task of covering children under their parents for up to twenty-
- 66. six years of age. These have deep fiscal implications that have the long-term impact on the companies. These have further long-term financial consequences to these enterprises. There is a need for flexibility, and without proper planning, most of these businesses may quickly run out of business based on the fact that they are not financially prepared for these changes. As of 2016 many of the newly established insurers have had to go into financial distress to the extent of failing and going out of business. The effect has also been seen in the larger companies such as United Healthcare which have so far withdrawn from the ACA’s exchange market due to the important financial losses that it had been facing. The insurers as of 2016 only managed to make only two percent of profits higher than the projected profits in 2010 even after the account reinsurance payment done. This is evidence of the deep financial plunges that insurance companies have had to deal with as a result of actions such as increasing the insurance cover limit. In conclusion, the new health care act has had a very great impact on the insurance companies. This range from fiscal implications to having to accommodate more people at a smaller cost than it was before. Many adjustments have therefore been made to accommodate these changes. The greatest impact of all time is that these companies have shifted focus from making more money from claims to ensuring that everybody gets an insurance policy or treated at a lower cost. These companies have often focused on making money for themselves at times compromising the health of the patients. These include situations such as dropping of patients due to complications developed so as to cut the costs of money discharged by the insurance companies. Much as there seem to be more negative impacts as opposed to the positive ones, the insurance companies may have ultimately been favored as they have more people to cover thereby accumulating more money while offering better services to the people. Finally, the ACA has enabled more companies to crop into the market thus creating equilibrium as more money has been allocated by the federal
- 67. government to support the provision of better health care for people. References Berwick, D. M., & Hackbarth, A. D. (2012). Eliminating waste in US health care. Jama, 307(14), 1513-1516. Blumenthal, D., & Collins, S. R. (2014). Health care coverage under the Affordable Care Act—a progress report. Cantor, J. C., Monheit, A. C., DeLia, D., & Lloyd, K. (2012). Early impact of the Affordable Care Act on health insurance coverage of young adults. Health services research, 47(5), 1773-1790. Protection, P., & Act, A. C. (2010). Patient protection and affordable care act. Pu Huntington, W. V., Covington, L. A., Center, P. P., Covington, L. A., & Manchikanti, L. (2011). Patient Protection and Affordable Care Act of 2010: reforming the health care reform for the new decade. Pain Physician, 14(1), E35-E67.blic Law, 111, 48. Rosenbaum, S. (2011). The Patient Protection and Affordable Care Act: implications for public health policy and practice. Public health reports, 126(1), 130- 135. Sommers, B. D., Gunja, M. Z., Finegold, K., & Musco, T. (2015). Changes in self-reported insurance coverage, access to care, and health under the Affordable Care Act. Jama, 314(4), 366-374.