ORAL MUCOSITIS easy ppt for Nurses
•
0 likes•75 views

ORAL MUCOSITIS definition incidence pathogenesis causes and risk factors clinical manifestations assessment management nursing management

Recommended
More Related Content
Similar to ORAL MUCOSITIS easy ppt for Nurses
Similar to ORAL MUCOSITIS easy ppt for Nurses (20)
More from Swatilekha Das
More from Swatilekha Das (20)
Recently uploaded
Recently uploaded (20)
ORAL MUCOSITIS easy ppt for Nurses
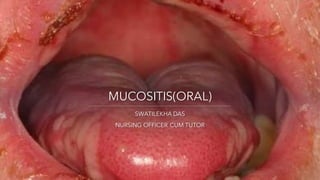
- 1. MUCOSITIS(ORAL) SWATILEKHA DAS NURSING OFFICER CUM TUTOR
- 3. MUCOSITIS(ORAL) • CT or RT induced ,painful inflammation and ulceration of the mucous membranes lining the GI tract. • Oral/oropharyngeal mucositis affects the keratinized mucosa of the dorsal tongue, gingiva, and /or hard palate; mucositis can also develop in the small intestine (GI mucositis) or the rectal mucosa (Proctitis). 3 SWATILEKHA DAS
- 4. • OM severity ranges from superficial erythema and soreness to full thickness mucosal ulcerations withy major pain, delayed , interrupted or discontinued treatment, systemic infections, hospitalization; impaired oral nutrition and economic burden. 4 SWATILEKHA DAS
- 5. Incidence • 20%-40% of patients receiving standard –dose CT • 60% -100% of those undergoing hematopoietic stem cell transplantation(HSCT) • and almost all patients receiving RT for HNC(>50% with grade 3 or 4) 5 SWATILEKHA DAS
- 6. • Mucositis involves epithelial mucosa, submucosal cells, and tissues and basal membrane. 6 SWATILEKHA DAS
- 7. Pathogenesis Initiation-within seconds of injury to highly proliferative , Nnormal cells & supporting connective tissues, DNA damage and other cellular responses lead to tissue changes. A primary damage response; transcription factors upregulate an innate response and activate expression of genes and multiple pathways, production of cytokines and modulators associated with the progression of mucositis. It becomes clinically apparent in the ulceration phase-loss of mucosal integrity ,painful lesions, submucosal breach with bacterial colonization and secondary infection. Healing occurs after CT or RT stopped.Submucosa and mesenchyme signal the mucosa to reepithelialize.The mucosa appears normal , but residual angiogenesis means increased risk for future mucositis episodes. 7 SWATILEKHA DAS
- 9. Causes and risk factors CT(cyclophosphamide, doxorubicin,vincristine,etoposide,ifosfamide, methotrexate,docetaxel, palitaxel,cisplatin,carboplatin,oxaliplatin,5-FU,leucovorin) RT for HNC Combined CT & RT increases risk to greater degree Baseline nutritional status below average –body mass index(BMI)-<18.5 9 SWATILEKHA DAS
- 10. Causes and risk factors Unintentional pretherapy weight loss (>5% over 1 month or >10% last 6 months) Poor oral hygiene, peridontal disease Persistent smoking or alcohol use Xerostomia Impaired renal function(high serum creatitine) may increase risk 10 SWATILEKHA DAS
- 11. Clinical manifestations A) Cycled or conditioning CT regimen- Mild erythema start 3- 4 days after CT;ulcers thereafter;peak intensity days 7 and 14; usually resolves in next week 11 SWATILEKHA DAS
- 12. B) RT for HNC • Oral mucosal erythema and soreness start around week 1 • Cumulative dose 20 to 30 Gy, frank ulcers; pain worsens, and oral intake decreases • Continued RT (to total 60-70 Gy );increased cumulative damage; difficult to control pain • OM typically resolves 2 to 4 weeks after RT completion, may persist longer. 12 SWATILEKHA DAS
- 13. C) Progressive ulcerative OM More diffuse, ulcers may be accompanied by : • Thick secretions that induce coughing, aspiration and disturb sleep • Pain that necessitates opioid analgesics • Impaired speaking, eating and drinking and swallowing • High risk gram negative bacterial or yeast infections and septic complications 13 SWATILEKHA DAS
- 14. Assessment • History- • Usual oral hygiene • Any changes in speaking, eating and drinking and swallowing • Screen for PCM • Use OM grading scale • Oral pain/comfort • Mouth dryness 14 SWATILEKHA DAS
- 15. • Use OM grading scale: World Health Organization Oral Mucositis Grading Scale 15 SWATILEKHA DAS
- 16. Physical examination • Recommended – regularly assess OM • Use a penlight to examine mouth for redness, swelling,ulcerations,white patches • Auscultatelung for potential for aspiration 16 SWATILEKHA DAS
- 17. Psychological assessment • Does sore mouth interfere with eating, drinking, talking; make them feel depressed • If they no longer enjoy the social interaction eating with others • If they act alone because it takes much longer to finish a meal than others • Imagery and laboratory tests : nothing specific to OM 17 SWATILEKHA DAS
- 18. Management • Medical - • Palifermin (keratinocyte growth factor)- food and drug administration(FDA) approved for patients with hematologic malignancy receiving high dose CT /total body irradiation, followed by autologous HCST; 60 microgram/kg body weight per day. 3 days before and after conditioning regimen(very costly) to reduce incidence and severity of OM 18 SWATILEKHA DAS
- 19. Supportive care drugs • Supportive care drugs- analgesics(Opioids and adjuvants) to relieve severe pain • >97% of pts with ulcerative OM require opioid analgesics(usually morphine equivalent) by week 4. Opioid doses increase to week 7 , usually needed for 6weeks after treatment completion. 19 SWATILEKHA DAS
- 20. Adding adjuvant analgesics may be opioid sparing: • Add gabapentin to analgesic regimen • Doxepin 0.5% mouthwash • Simple or niosomal amitryptyline mouthwash or benzydamine(NSAID mouthwash 15ml, swish 30 seconds and spit), provide temporary pain relief. 20 SWATILEKHA DAS
- 21. Low level laser therapy Biweekly or weekly- reduces OM prevalence, severity , duration and associated pain 21 SWATILEKHA DAS
- 22. Research studies • Instruct pt to hold ice chips in mouth for 5 minutesbefore CT or RT , during CT or RT, and after 30minutesafterwards • Very helpful 5 FU and high dose melphalan;inconclusiveresults- methotrexate, etoposide, cisplatin,mitomycin,vinblastine • Contraindicatedwith oxaliplatin because of risk for laryngeal dysesthesia. 22 SWATILEKHA DAS
- 23. Nursing management • Preventive oral care- Pretreatment and dental examination and instruction for oral hygiene regimen 23 SWATILEKHA DAS
- 24. Nursing management • Remind pts about helpful dietary tips for painful OM, avoid spicy foods, hot foods and rinks, eat soft or moistened foods. 24 SWATILEKHA DAS
- 25. Nursing management Topical protective /coating agent: • Benzocaine (ora-base, Oratect gel, hurricaine)+- analgesics(e.g. viscous lidocaine, magic mouthwash) may give some temporary relief. 25 SWATILEKHA DAS
- 26. Nursing management • Use of normal saline, salt and baking soda(0.5 tea spoon each in 1 cup of warm water) ; or plain water rinses. 26 SWATILEKHA DAS