
Recommended
Recommended
More Related Content
Viewers also liked
Viewers also liked (20)
Similar to Diadetic foot
Similar to Diadetic foot (20)
Recently uploaded
Recently uploaded (20)
Diadetic foot
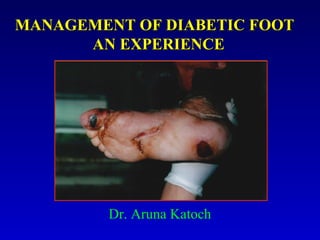
- 1. MMAANNAAGGEEMMEENNTT OOFF DDIIAABBEETTIICC FFOOOOTT AANN EEXXPPEERRIIEENNCCEE Dr. Aruna Katoch
- 2. INTRODUCTION Diabetic population of the world is 5 crore seventy lacs out of 17 crore i.e. 1/3 of the total population of the diabetics belongs to India. The diabetic foot is still a problem of first not only for the quality of life of affected patient but also to society due to its high cost. And only preventive measures are know to lower down the risk for amputation of 60-80%. This falls under the heading of PRAMEHA PIDIKA – the major complication of Prameha.
- 3. PIDIKA SAMPRAPTI “r= olkesnksH;kefHkiUu’kjhjL; f=fHknksZÔS’pkuqxr/kkrks% çesfg.kks n’k fiMdk tk;UrsA” In the patient of prameha when the body is permeated by vasa and medas and dhatus are affected by three dosas, ten boils appears.
- 4. STHANA (SITE) jlk;uhuka p nkScZY;kUuks/oZeqfUr"BfUr çesfg.kka nks"kk%] rrks e/kqesfgUkke/k% dk;s fiMdk % çknqHkZofUr Susruta has mentioned in twelveth chapter of Chikistasthana that due to atony of Lymphatics (jlk;uhuka) in patient of prameha, dosas do not move upwards and as such boils appear in the lower parts of the
- 5. AETIOLOGY • Peripheral sensory neuropathy • Trauma • High Planter Pressures FEATURE • Most characteristic lesion of Diabetic Foot is a mal perforans ulceration
- 6. CLASSIFICATION Modern : Wagner Ulcer Classification System: Grd Lesion 0 No open lesions; may have deformity or cellulitis 1. Superficial diabetic ulcer (partial or full thickness) 2. Ulcer extension to ligament, tendon, joint capsule or deep fascia without abcess or osteomyelitis 3. Deep ulcer with abcess, osteomyelitis or joint sepsis 4. Gangrene localized to portion of forefoot or heal. 5. Extensive gangrenous involvement of the entire foot. American Family Physician AYURVEDIC : Saravika, Sarsapika, Kacchapika, Jalini, Vinata, Putrini, Masurika, Alaji, Vidarika, Vidradhika Su.Ni-6/15-19
- 7. TREATMENT For this Multidisciplinary management is advised Rest, elevation of the affected foot & relief of pressure ¯ TCC is advised (Total contact casting) ¯ Debridement of all necrotic, callus & fibrous tissue ¯ If wound is Healthy Unhealthy ¯ This leads towards gangrene or osteomyelitis ¯ Hospitalization for surgical drainage ¯ Skin grafting is done for deep If healthy Ulcer as its repair ¯ Amputation
- 8. TREATMENT IN AYURVED According to Susruta Samphita First Nine out of Ten boils are Sadhya i.e. Saravika to Vidarika. But treatment for all of them is described in seven step as follows: • Stage Treatment • Apakva Pidika Shophvat Chikitsa • Pakva Pidika Vranvat Chikitsa • Ropanarth Use of medicated oil • Utsadanarth Aargwadadi Kshayam • Parishecanarth Salsaradi Kshayam • Paan-Bhojanadi Pippaladi Kshayam • Prasanarth Patadi Churan Su.Chk.12/9
- 9. CASE PRESENTATION & CLINICAL EVALUATION • 70 yrs male suffering from diabetic foot ulcer from April, 2004, came to us on 8th July, 2004 with diagnosed D.M with large sized abscess on the sole of the right foot with cellulitis of the dorsum. He was on inj. Insulin from last 3 months INVESTIGATIONS • FBS = 80mg/dl., • Glycosylated Haemoglobin was under fair control. • X-rays showing extensive bony destruction with osteolytic area involving phalanges of great toe and head of first metatarsal.
- 10. EXAMINATION (i) Number of Wound = 3 (ii) Location with size: (1) Great toe along with top of plantar surface of sole of the foot. 3 cm x 2 cm (toe) 8 cm x 5 cm (over sole) (2) Middle of foot = 5 cm x 1 cm (3) Heel (Diameter) = 3 cm x 0.5 cm. 1 2 3
- 11. MATERIAL AND METHOD Drug selected for study: 1. Paradadi churan(churan of impure parad, ghandhak, • kapur, sangjarahath, and pure neelatotha from Rastantarsaar) 2. Jatayadi tail (Bh.R.)and Nirgundi tail(Sh.S)
- 12. TREATMENT SCHEDULE Treatment was planned under two phases as per treatment principle of Susruta Samhita for Prameha Ppidika . (i) Vranvat Chikitsa with Paradai Churan till granulation appeared. (ii) Ropan Chikitsa with Nirgundi Tail and Jatayadi tail when granulation tissue had formed. (iii) For controlling diabetes insulin was remained as advised earlier. (iv) Immunity enhances was also given in form of oral medication
- 13. PROCEDURE FOR DRESSING (i) For ten days, antiseptic dressing was done twice a day with a paste of Paradadi Churan + Jatayadi Tail after washing with saline water. Every time slough and debris was removed. There was abcess underneath the nail. So the nail was removed and osteoporotic pieces of bone were also removed. (ii) After ten days, dressing with Jatayadi Tail and Nirgundi Tail was started which is continued till now. (iii)After wound was healed for 3 cms. beneath the second and third toes upto great toe it was observed that due to formation of fibrous tissue the edge of the wound were a part so both the edges were approximated by making the area raw with lekhen karma and then suturing was done.
- 14. CHRONOLOGY OF CLINICAL OBSERVATION (i) Patient was brought to OPD on 08.07.2004 with minor gangrene of great toe and other three wounds discussed above. (ii) Patient was subjected to above scheduled treatment and kept under regular observation. (iii)After ten days, the gangrened area and the foul smell of the wound disappeared, slough formation was reduced, nocturnal pain disappeared, odema was reduced. But size of the great toe shortens due to removal of osteportic bone pieces and nail. Temp. was 99.4 F. There was formation of granulation issue on the wound no.1 and 2 whereas wound no.3 was completely healed. The FBS was 110 mg/dl.
- 15. (iv) After one and half month, there was no slough formation, no pain, Temp. was normal, slight odema of feet was present. The value of F.B.S. is 101 mg/dl. and the size of wound 1 was reduced to 5 cm x 4 cm (8 cm x 5 cm earlier). Size of wound 2 was reduced 2 cm x 1 cm (5 cm x 1 cm earlier). (v) After 18 days, size of the wound 1 was reduced to 4cm x 2cm. But the edges of the wound were apart because of formation of callus tissue over remained 3 cms. So, both edges of the wound were approximated by making them raw and then sutured with Mercisilk 3-0.
- 16. (iv) After next 12 days stitches of the wound were removed and observed that area was healed completely and the wound remained 3 cm x 1 cm only whereas wound 2 was healed completely as in photograph 2. 1 2 3 1 2 Photograph 2A Photograph 2B
- 17. vi) Now dressing of wound no.1 is still continued. Photograph 3A Photograph 3B
- 18. DISCUSSION AND COMMENTS • Diabetic foot ulcer associated with gangrene of localized are of great toe is a challenging problem in day to day clinical practice as it comes under the category of Grade 4 according to Wagner Ulcer Classification System. The current medical management is unsatisfactory as drugs which limit inflammation, such as non-steroidal anti-inflammatory or steroids will slow the healing of a wound as it hinders the first phase of healing i.e. inflammation. Secondly, the preparatory solutions used for cleaning the wound, such as iodide, peroxide or strong detergents will cause harm than good as not only they kill bacteria but they also kill fibroblasts and epithial cells (second phase of healing). Deeply pigmented solutions can alter a wound’s appearance, making it more difficult to determine tissue viability. So, only balanced salt solution is entirely appropriate and then surgical intervention is only the option i.e. amputation. www.plasticsurgery.com
- 19. • On the other hand, Paradadi Churan which is a Herbomineral component increases the blood supply as well as Bio-chemical ingredients needed for healing of the affected area. So there is increase in leukocyte and monocytes for bacterial phagocytosis and lysis fibrogen for adherence of wound; histamine, prostaglandins and vesoactive substances for haemostasis. So with Paradadi Churan first phase of healing becomes faster. Jatayadi Tail looks after for bacterial contamination and odema and Nirgundi tail increases the epitheliazation. Both together reduces the callus formation and enhance wound contraction by migration of epithelium from wound margins to centre. Neither epithelial migration nor contraction will proceed in the presence of heavy bacterial contamination. Both oils is of special significance of course maintaining asepsis is of immense importance. With this I would like conclude that Susruta has mentioned wonderful treatment for Prameha Pidika which is followed by Ayurvedic Practitioners for Management of Foot Ulcers whereas in Allopathic Treatment amputation is done.
- 20. At last “We cared for the wound; but God healed it”.