This document outlines the key components and structure for taking a thorough pediatric history, including:
1) Active listening techniques and types of questions to facilitate the interview.
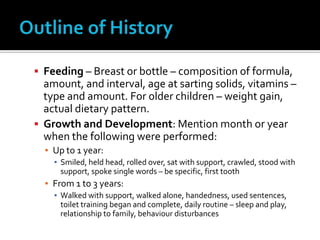
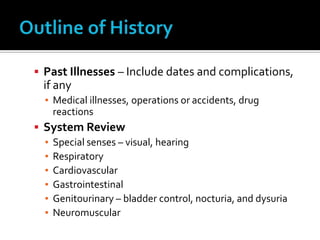
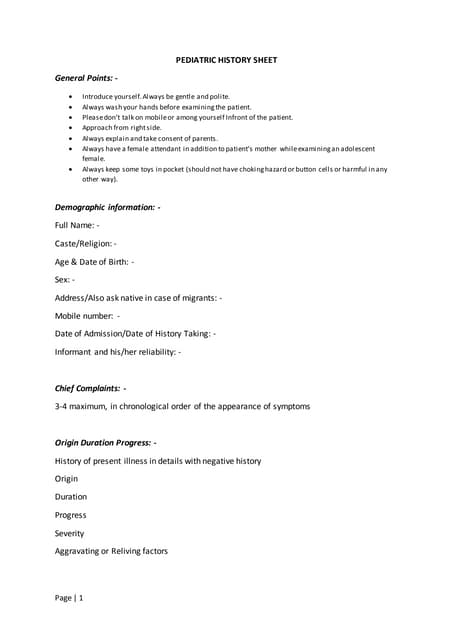
2) The outline should include information on the chief complaint, present illness, family history, social context, personal history of prenatal/birth, development, behaviors, immunizations and past illnesses.
3) It also describes taking an interval history if the patient has been hospitalized before to understand their condition between admissions.