
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Mechanical Ventilation
Similar to Mechanical Ventilation (20)
Recently uploaded
Recently uploaded (20)
Mechanical Ventilation
- 1. Sonali & Rachana 1
- 2. Mechanical Ventilation Prepared By- Sonali Koiri Rachana Shrestha BNS 3rd Year
- 3. Contents 1. Introduction of Mechanical Ventilation 2. Goals of Mechanical Ventilation 3. Indication of Mechanical Ventilation 4. Criteria for institution of Mechanical Ventilation 5. Introduction of Mechanical Ventilator and its parts 6. Common ventilator settings 7. Classification of ventilation 8. Modes of ventilation 9. Nursing Management of patient in mechanical ventilation Sonali & Rachana 3
- 4. Introduction Mechanical Ventilation: The mechanical ventilation is the process by which gas is moved into the lungs by creating a pressure gradient artificially. Respiratory support is needed to correct hypoxemia and hypercapnia and to reduce work of breathing. Sonali & Rachana 4
- 5. Goals • Treat hypoxemia. • Treat acute respiratory acidosis. • Relief of respiratory distress. • Prevention or reversal of atelectasis. • Resting of ventilatory muscles. Sonali & Rachana 5
- 6. Indications • Neurological impairment (drugs, poisions , snake bite, trauma) with “Glasgow Coma Scale “ (GCS) ≤ 8. • Respiratory Failure a. Arterial PaO2 <60 mm Hg (on supplemental Oxygen). b. Arterial PaCO2 >50 mm Hg (in the absence of chronic airway disease) Sonali & Rachana 6
- 7. Contd c. Evidence of elevated work of breathing: Respiratory rate > 35 breaths/minute. Tidal volume < 5ml/kg. Vital Capacity < 15ml/kg. Presence of retraction or nasal flaring. Paradoxical or divergent chest motion. • Cardiopulmonary arrest. • Neuromuscular disorders. • Lung Diseases. Sonali & Rachana 7
- 8. Criteria for institution of ventilatory support: Normal range Ventilation indicated Parameters 10-20 5-7 65-75 75-100 > 35 < 5 < 15 <20 A- Pulmonary function studies: • Respiratory rate (breaths/min). • Tidal volume (ml/kg body wt) • Vital capacity (ml/kg body wt) • Maximum Inspiratory Force (cm HO2)
- 9. Cont.. Normal range Ventilation indicated Parameters 7.35-7.45 75-100 35-45 < 7.25 < 60 > 50 B- Arterial blood Gases • PH • PaO2 (mmHg) • PaCO2 (mmHg)
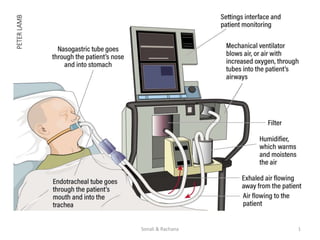
- 10. Introduction Mechanical Ventilator: • A mechanical ventilator is a positive or negative pressure breathing device that can maintain ventilation and oxygen delivery for a prolong period. • It is a machine that generates a controlled flow of gas into a patient’s airway. 10Sonali & Rachana
- 11. Sonali & Rachana 11
- 13. Monitor/ Screen
- 14. Heat & Moisture Exchanger (HME) Filter
- 15. Contd…
- 16. Humidifier
- 17. Flow Sensor
- 19. Catheter Mount
- 21. Common Ventilator Settings parameters/ controls • Fraction of inspired oxygen (FIO2) • Tidal Volume (VT) • Peak Flow/ Flow Rate • Respiratory Rate/ Breath Rate / Frequency ( F) • I:E Ratio (Inspiration to Expiration Ratio) • PEEP
- 22. Fraction of inspired oxygen (FIO2) • The percent of oxygen concentration that the patient is receiving from the ventilator. (Between 21% & 100%) • Initially a patient is placed on a high level of FIO2 (60% or higher). • Subsequent changes in FIO2 are based on ABGs and the SaO2. • The lowest possible fraction of inspired oxygen (FiO2) necessary to meet oxygenation goals should be used.
- 23. Tidal Volume (VT) • The volume of air delivered to a patient during a ventilator breath. • The amount of air inspired and expired with each breath. • Usual volume selected is between (5 to 15 ml/ kg body weight) • In the volume ventilator, Tidal volumes of 10 to 15 mL/kg of body weight were traditionally used. • The large tidal volumes may lead to (volumtrauma) aggravate the damage inflicted on the lungs. • For this reason, lower tidal volume targets (6 to 8 mL/kg) are now recommended.
- 24. Respiratory Rate/ Breath Rate / Frequency ( F) • The number of breaths the ventilator will deliver/minute (10-16 b/m). • Total respiratory rate equals patient rate plus ventilator rate. • An optimal method for setting the respiratory rate has not been established. For most patients, an initial respiratory rate between 12 and 16 breaths per minute is reasonable • The nurse double-checks the functioning of the ventilator by observing the patient’s respiratory rate.
- 25. Positive End-Expiratory Pressure (PEEP) • PEEP is the pressure in the lungs (alveolar pressure) above atmospheric pressure (the pressure outside of the body) that exists at the end of expiration. • Applied PEEP is generally added to mitigate end- expiratory alveolar collapse. A typical initial applied PEEP is 5 cmH2O. However, up to 20 cmH2O may be used in patients undergoing low tidal volume ventilation for acute respiratory distress syndrome (ARDS).
- 26. Peak Flow/ Flow Rate • The velocity of gas flow or volume of gas delivered by the ventilator per minute (L/min) • The higher the flow rate, the faster peak airway pressure is reached and the shorter the inspiration; • The lower the flow rate, the longer the inspiration.
- 27. I:E Ratio (Inspiration to Expiration Ratio) • During spontaneous breathing, the normal I:E ratio is 1:2, indicating that for normal patients the exhalation time is about twice as long as inhalation time. • If exhalation time is too short “breath stacking” occurs resulting in an increase in end-expiratory pressure also called auto-PEEP.
- 28. CLASSIFICATION • Negative Pressure Ventilation • Positive Pressure Ventilation Volume Controlled Pressure Controlled Sonali & Rachana 28
- 29. Negative Pressure Ventilation • These exert negative pressure on external chest decreasing the intra-thoracic pressure during inspiration, allows air to flow into the lungs, filling its volume. • These are simple to use and do not require intubations of the airways; consequently, they are especially adaptable for home use. • It is used mainly in chronic respiratory failure associated with neuromuscular conditions. Sonali & Rachana 29
- 30. Contd • Examples: Iron lung, body wrap and chest cuirass • Disadvantages Limited access for patient care Inability to properly monitor pulmonary mechanics Patient discomfort
- 31. Positive Pressure Ventilation • A positive pressure ventilation inflate the lungs by exerting positive pressure in the airway forcing the alveoli to expand during inspiration. Expiration occurs passively. • It requires an artificial airway (endotracheal or tracheostomy tube) and use positive pressure to force gas into patient’s lungs. • Inspiration can be triggered either by the patient or machine.
- 35. Classification of Positive Pressure Ventilation 1. Volume controlled Deliver a preset tidal volume Allows pressure to vary with changes in resistance and compliance Volume delivery remains constant 2. Pressure controlled Deliver a preset inspiratory pressure during each inspiration Volume delivery may vary 35
- 36. Pressure and Gradients • Peak inspiratory pressure (Ppeak) • Plateau pressure (Pplateau) • Baseline pressure • Mean airway pressure (Pmean) 36
- 38. PHASES OF VENTILATORY CYCLES 1. TRIGGERING (Initiation of inspiration) 1. INSPIRATION 2. CYCLING (Change over from inspiration to expiration) 3. EXPIRATION CONTROL VARIABLE 1. PRESSURE (cm H2O) 2. FLOW (L/min) 3. VOLUME (ml) 4. TIME (sec)
- 40. Modes of Mechanical Ventilation 40
- 41. Selection of Modes of Ventilation Regardless of which operating mode is selected, it should achieve four main goals: • Provide adequate ventilation and oxygenation. • Avoid ventilator-induced lung injury. • Provide patient-ventilator synchrony. • Allow successful weaning from mechanical ventilation. 41
- 42. Modes • Continuous mandatory mode – Control (CMV) – Assist control (AC) • Intermittent Mandatory mode – IMV (Intermittent Mandatory Ventilation) – SIMV ( synchronized Intermittent Mandatory Ventilation) • Spontaneous mode – Continuous Positive Airway Pressure (CPAP) – BiLevel Positive Airway Pressure (BiPAP) 42
- 43. Controlled Mandatory Ventilation (CMV) The ventilator initiates and controls both the volume delivered and the frequency of breaths. Patient cannot trigger ventilation. Patient should be sedate and possibly paralyzed. This mode is used for the patient who is unable to initiate breath. Not often used in ICU as it does not allow any synchronisation with the patient's own breathing 43
- 44. CMV 44
- 45. Contd… Advantages • Guaranteed volume(or pressure ) with each breath • Low patient workload Disadvantages • Spontaneous breath not allowed • Needs deep sedation & Paralysis • Apnea & Hypoxia if accidentally disconnected • Ventilator dependence 45
- 46. Assist Control Mode (AC) Assist-control ventilation allows the patient to initiate a ventilator breath (assisted or patient-triggered ventilation), but if this is not possible, ventilator breaths are delivered at a preselected rate (controlled or time- triggered ventilation). The ventilator breaths during ACV can be volume- controlled or pressure-controlled. Used for the patients who can initiate a breath but who have weakened respiratory muscles such as Gullain Barre Syndrome, post cardiac or respiratory arrest, pulmonary oedema, ARDS etc. 46
- 47. AC mode 47
- 48. Contd… Advantages • Increase Patients comfort • Patients work of breathing is low • Patient can control the frequency Disadvantages • Risk of Hyperventilation 48
- 49. Intermittent Mandatory Ventilation Intermittent mandatory ventilation provides a combination of mechanical breaths and spontaneous breaths . Mechanical breaths are delivered at preset intervals and a preselected tidal volume, regardless of patient’s efforts. Patient is allowed to breath independently except during certain prescribed intervals. 49
- 50. IMV 50
- 51. Contd… Advantages • Allows spontaneous breath of any tidal volume Disadvantages • Increase work of breathing • Asynchrony 51
- 52. Synchronized Intermittent Mandatory Ventilation (SIMV) SIMV also delivers a preset tidal volume and number of breaths per minute . Between ventilator delivered breaths the patient can breath spontaneously. Mandatory breaths are synchronised with the patient's own inspiratory effort which is more comfortable for the patient 52
- 53. Contd… Advantages • The mandatory breath is delivered in synchrony with patient effort. This makes greater comfort during breathing. • The patients respiratory muscles remain active, and so disuse atrophy is less common. Disadvantages • Hypoventilation is possible if the patient is not capable of spontaneous breathing. • Excessive work of breathing is possible during spontaneous breaths unless an adequate level of pressure support is applied. 53
- 54. Spontaneous mode 1. Continuous positive airway pressure(CPAP) 2. Noninvasive bilevel positive airway pressure ventilation (BiPAP)
- 55. Continuous Positive Airway Pressure (CPAP) Constant positive airway pressure during spontaneous breathing This is a mode and simply means that a preset pressure is present in the circuit and lungs throughout both the inspiratory and expiratory phases of the breaths. CPAP serves to keep alveoli from collapsing, resulting in better oxygenation and less work of breathing. It is very commonly used as a mode to evaluate the patients readiness for weaning or extubation. CPAP can be used for intubated and nonintubated
- 56. CPAP cont… • The purpose of CPAP is to improve and support the patient’s oxygenation. CPAP does not improve the patient’s ventilatory status, so the patient must be breathing spontaneously if CPAP is in use. • Indication: • Hypoxemic respiratory failure • Obstructive sleep apnea • Congestive heart failure • Weaning from ventilation
- 57. Bilevel Positive Airway Pressure Ventilation (BiPAP) • BiPAP is a noninvasive form of mechanical ventilation provided by means of a nasal mask or nasal prongs, or a full-face mask. • The system allows the clinician to select two levels of positive-pressure support: • An inspiratory pressure support level (referred to as IPAP) • An expiratory pressure called EPAP .
- 58. BiPAP cont.. • BiPAP can help to improve the patient’s ventilatory status. So if the patient has an elevated PaCO2, BiPAP can be administered in order to help decrease the PaCO2 back into the normal range. • Indication • Hypercapnic respiratory failure • Acute respiratory failure • COPD • Heart failure
- 60. Complications of mechanical ventilation • Infections/Ventilator associated pneumonia(VAP) • Lung Damage/ Pulmonary barotrauma • Pneumothorax • Pulmonary edema • Tracheal stenosis • Hypoxemia • Delirium • Immobility • Vocal cord problems • Gastrointestinal problems(paralytic ileus, stress ulcer)
- 61. Methods of Weaning T-piece trial Continuous Positive Airway Pressure (CPAP) weaning Synchronized Intermittent Mandatory Ventilation (SIMV) weaning
- 62. Synchronized Intermittent Mandatory Ventilation ( SIMV) Weaning • SIMV is the most common method of weaning. • It consists of gradually decreasing the number of breaths delivered by the ventilator to allow the patient to increase number of spontaneous breaths
- 63. Continuous Positive Airway Pressure (CPAP) Weaning • When placed on CPAP, the patient does all the work of breathing without the aid of a back up rate or tidal volume. • No mandatory (ventilator-initiated) breaths are delivered in this mode i.e. all ventilation is spontaneously initiated by the patient. • Weaning by gradual decrease in pressure value
- 64. T-Piece trial • It consists of removing the patient from the ventilator and having him / her breathe spontaneously on a T- tube connected to oxygen source. • During T-piece weaning, periods of ventilator support are alternated with spontaneous breathing. • The goal is to progressively increase the time spent off the ventilator.
- 65. T-Piece
- 66. Role of nurse before weaning:- • Ensure that indications for the implementation of Mechanical ventilation have improved • Ensure that all factors that may interfere with successful weaning are corrected:- - Acid-base abnormalities - Fluid imbalance - Electrolyte abnormalities - Infection - Fever - Anemia - Sleep deprivation
- 67. Role of nurse before weaning:- • Assess readiness for weaning • Ensure that the weaning criteria / parameters are met. • Explain the process of weaning to the patient and offer reassurance to the patient. • Initiate weaning in the morning when the patient is rested. • Elevate the head of the bed & Place the patient upright • Ensure a patent airway and suction if necessary before a weaning trial, • Provide for rest period on ventilator for 15 – 20 minutes after suctioning.
- 68. Cont… • Ensure patient’s comfort & administer pharmacological agents for comfort, such as bronchodilators as indicated. • Help the patient through some of the discomfort and apprehension. • Support and reassurance help the patient through the discomfort and apprehension as remains with the patient after initiation of the weaning process. • Evaluate and document the patient’s response to weaning.
- 69. Role of nurse during weaning:- • Wean only during the day. • Remain with the patient during initiation of weaning. • Instruct the patient to relax and breathe normally. • Monitor the respiratory rate, vital signs, ABGs, diaphoresis. If signs of fatigue or respiratory distress develop. • Discontinue weaning trials.
- 70. Role of nurse after weaning 1- Ensure that extubation criteria are met . 2- Extubate 2- Documentation
- 71. Nursing care of patients on ventilator 1. Check ventilator setting and modes • When you enter the patient’s room, take vital signs, check oxygen saturation , listen to breath sounds and note changes from previous findings. Also assess the patient’s pain and anxiety levels. Compare current ventilator settings with the setting prescribed in the order • Suctioning for airway clearance. • Chest physiotherapy and breathing exercise for secretions mobilization
- 72. Nursing care of patients on ventilator 2. Communication • Assessment of the ability of the ventilator- dependent patient to communicate • Use non verbal methods of communication • Be alert to non verbal clues. • Use of signals, signs, nodding, palms, writing, lip reading • Provide paper and pencil, magic slate • Allow patient to respond and repeat explanations • Ask simple yes/no questions to which she can nod or shake her head.
- 73. Cont… 3. Management of airway Assess respiratory rate and depth inspect thorax for symmetry of movement Observe for SOB Assess the patient for oxygenation such as oxygen saturation, signs and symptoms of hypoxia( tachypnea, nail beds, ABGs analysis and auscultation for air entry) Elevate head of bed 60-90 degree. • Humidification of the airway through the ventilator to help to liquefy the secretions for easy removal • Use of bronchodilators • Administration of mucolytics to liquified
- 74. Cont… 4. Suctioning Suction appropriately Suction only as needed not according to a schedule. Hyper oxygenate the patient before and after suctioning to help prevent oxygen desaturation Limit suctioning pressure to the lowest level needed to remove secretions. Suction for the shortest duration possible.
- 75. Cont… 5. Ensuring humidification and thermoregulation • All air delivered by the ventilator passes through the water in the humidifier, where it is warmed and saturated. • Humidifier temperatures should be kept close to body temperature 35 ºC- 37ºC. • In some rare instances (severe hypothermia), the air temperatures can be increased. • The humidifier should be checked for adequate water levels • An empty humidifier contributes to drying the airway, often with resultant dried secretions, mucus plugging
- 76. Cont… • Humidifier should not be overfilled as this may increase circuit resistance and interfere with spontaneous breathing. • As air passes through the ventilator to the patient, water condenses in the corrugated tubing. This moisture is considered contaminated and must be drained into a receptacle and not back into the sterile humidifier. • If the water is allowed to build up, resistance is developed in the circuit and PEEP is generated. In addition, if moisture accumulates near the endotracheal tube, the patient can aspirate the water. • The nurse and respiratory therapist jointly are responsible for preventing this condensation buildup. The humidifier is an ideal medium for bacterial growth.
- 77. Cont… 6. Ventilator alarms • Mechanical ventilators comprise audible and visual alarm systems, which act as immediate warning signals to altered ventilation. • Alarm systems can be categorized according to volume and pressure (high and low). • High-pressure alarms warn of rising pressures. • Low-pressure alarms warn of disconnection of the patient from the ventilator or circuit leaks.
- 78. Cont… 7. Management of fluid imbalances Assessment of the patient including presence of edema, intake and output charting, signs and symptoms of dehydration. Planning of fluid administration carefully Central venous pressure monitoring as well as measuring cardiac output.
- 79. Cont… 8. Prevention for pulmonary infection Provide good oral care Suction when need indicated using sterile technique. Handwashing with antimicrobial for 30 seconds before and after patient contact Use sterile saline for suctioning Ensuring ventilator tubing changed between patients and whenever become solled
- 80. Cont… 9. Oral hygiene Oral care frequently because the oral cavity is the primary source contamination of the lungs in the intubated and compromised patients Provide oral care every 2 hourly as oral mucus membranes dry in 2 hours
- 81. Cont… 10. Maintain nutrition Assessment of the patient( serum protein) Assess bowel sounds Provide naso-gastric tube feeding. The naso- gastric tube can increase the risk of aspiration , leading to nosocomial pneumonia hence the patient should be positioned with the head elevated above the stomach. Parental nutrition if patient cannot tolerate orally Avoid too much carbohydrate feeds as it may increases CO2 production and may cause hypercapnia.
- 82. Cont… Prevention of bed sore Observe skin integrity for presssure ulcers. Preventative measures include turning patient at least 2 hourly. Use pressure relief mattress for bed if indicated. Educating family Explain purpose and all treatments Provide alternative method of communication. Elimination care Catheter care Proper cleaning, use of bed pans if possible Promoting coping ability
- 83. Cont… 12. Provide rest and sleep Keep calm and quiet environment. Turn monitor alarm down if possible Provide dim light during night and soft music Cover patient eyes with clean gauze. 13. Safety and security needs Prevent cross infection and nosocomial infection. Maintain warm and adequate body temperature Put side rails Visiting hours should be define
- 84. Cont… 14. Prevention of contractures Maintain muscles strength with active/passive ROM and prevent contractures with use of splint.
- 85. Noninvasive Positive Pressure Ventilation (NIPPV) • Noninvasive Positive Pressure Ventilation (NPPV) is medical procedure that involves the use of ventilatory support without using an invasive artificial airway such as endotracheal tube or tracheostomy tube. • During NPPV, the health care provider administers air, usually with added oxygen, through a face mask or nasal mask under positive airway pressure (external lung pressure being greater than the pressure inside of the lungs).
- 88. Benefits of NIPPV • Adequate ventilation and oxygenation • Correction of respiratory failure • Adequate patient tolerance and comfort • Makes activities of daily living easier because it helps patients use more of their lung capacity while decreasing the breathing work load. • Alleviates a wide array of symptoms such as daytime fatigue, breathing difficulties, and other symptoms associated with low oxygen levels. • It reduces length of hospital stay by providing clients with adequate ventilation while preventing respiratory failure. • It’s more convenient compared to invasive ventilation • It provides greater flexibility in the initiation and removal of
- 89. Indication • Acute respiratory failure • Acute severe asthma • Acute heart failure • Breathing impairment due to a spinal cord injury • COPD exacerbations • Chest wall disorders • Moderate acidemia (pH <7.35) • Moderate hypercarbia • Neuromuscular disease • Nocturnal hypoventilation • Prevention of reintubation in high-risk patients • Tachypnea • DNI(Do not intubate) order
- 90. Contraindication • Agitation or lack of cooperation • Excessive oral and nasal secretions • Inability to fit the mask • Inability to maintain a patent airway or protect the airway • Respiratory arrest
- 91. Complication • Aerophagia (excessive air swallowing) • Airway dryness • Aspiration • Claustrophobia • Dry mouth • Eye irritation from an air leak • Gastric distension and insufflation • Pressure areas from mask, tubing and strapping • Secretion build up inside the mask
- 92. References • https://www.slideshare.net/doctorshalinigarg/mechanical-ventilation- 3355414 • https://www.slideshare.net/bibinibaby5/mechanical-ventilation-ppt • https://www.slideshare.net/Harshita89/ventilators-32613130 • https://www.aafp.org/afp/2004/0801/p596.html • http://www.sle.co.uk/files/library/files/PDFs/howto/How%20to%20clean %20your%20ventilators.pdf • http://www.en.carefusion.com.br/documents/international/guides/user- guides/RC_VELA-Operator-Manual_UG_EN.pdf • http://rtasap.com/ppt/vela.pdf • https://ann-clinmicrob.biomedcentral.com/articles/10.1186/1476-0711-5- 7 • https://www.sciencedirect.com/science/article/pii/0002934384905205 • https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3647488/
Editor's Notes
- used to measure gas flows in ventilator.
- Prevents patient from fighting the ventilator, reducing need for sedation and paralysis Pressure support can be added to the spontaneous breath to overcome circuit and endotracheal tube resistance and unload inspiratory muscle work