
Recommended
More Related Content
What's hot
What's hot (20)
Similar to destructive operation (1).pptx
Similar to destructive operation (1).pptx (20)
Recently uploaded
Recently uploaded (20)
destructive operation (1).pptx
- 2. Destructive operations are procedure that reduce the size of the head , shoulder girdle, or trunk of the dead fetus to allow its delivery through the vaginal route… • To reduce baby’s size head girdle or body and so enable the vaginal delivery of baby which is too large to pass intact through the birth canal. • Operations that are designed to diminish the bulk of the fetus so as to facilitate delivery through the birth canal. DEFINE: PURPOSES : • Needs few instrument and simple anaesthesia • Uterus remains intact no LSCS • Subsequent pregnancy will be safer • Operative morbidity is lesser • Hospital stay is shorter
- 3. CONTRAINDICATION: • Living normal fetus • Markedly contracted pelvis • Cervix less than ¾th dilated • Neoplasm obstructing the pelvis CLASSIFICATION : • Living fetus • Dead fetus • Perforators • Smellie’s perforator • Simpson spring loaded perforator • Hooks / crochets • Cranioclast • Ramsbothams decapitating hook
- 4. CRANIOTOMY DECAPITATION EVISCERATION CLEIDOTOMY TYPES:
- 5. It is the operation to make a perforation on the fetal head to evacuate the contents followed by extraction of the fetus INDICATION: • Cephalic presentation producing obstructed labor with dead fetus… • Hydrocephalus even in a living fetus.. • Interlocking head of twins.. • Specifically unfavourable position of child impacted mento posterior ,brow or occipito posterior positions following a prolonger labour… CRANIOTOMY: PRE TREATMENT: • Correct dehydration • Treat keto acidosis • Draw blood for cross matching , investigations • To arrange blood • Catheterise the bladder
- 6. PROCEDURE: PRELIMINARIES: • Anaesthesia either general or local • Lithotomy position • Full surgical asepsis • Empty the bladder • Vaginal examination…
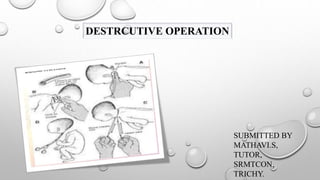
- 7. Step : 1 • The two fingers are introduced into the vagina and the finger tips are to be placed on proposed site of perforation… • However when the suture line cannot be defined because of big caput , the perforation should be done through the dependent part • Sites of preparation • Vertex : on the parietal bone either side of the sagittal suture is avoided to prevent collapse of the bone there by preventing escape of the brain matter • Face: through the orbit hard palate… • Brow: through the frontal bone…
- 8. STEP :2 The Oldham's perforator with the blades closed is introduced under the palmer aspects of the fingers protecting the anterior vaginal wall and the adjacent bladder until the tips reaches the proposed site of perforation.
- 9. • By rotating movements the skull is perforated… • During this step an assistant is asked to steady the head per abdomen in a manner of first pelvic grip… • After the skull is perforated the instrument is thrust up to the shoulder and the handles are approximately to as to allow separation of the sharp blades for about 2.5cm…. STEPS:3
- 10. STEP:4 With the fingers brain matter is evacuated . The idea is to make the skull collapse as much as possible … Step :5 When the skull is found sufficiently compressed , the extraction of the fetus is achieved either by using a cranioclast or by 2 giant valsella… Giant valsella are used to hold the incised skull and scalp margins… STEP:6 The traction is now exerted Step:7 After the delivery of the placenta , the uterovaginal canal must be explored as a routine for evidence of rupture uterus or another.. Inj. Methergin 0.2mg IM given with the delivery of anterior shoulder The rest of the delivery is completed as in normal delivery.
- 11. DECAPITATION: It is the destructive operation where by the fetal head is servered from the trunk and the delivery is completed with the extraction of the trunk and that of the decapitated head per vagina. INDICATIONS: • Neglected shoulder with a dead fetus • Locked twins • Double headed monsters…. • Pre requisites: • Neck of the fetus should be accessible per vagina • No evidence of impending rupture • Cervix should be at least 7cm dilated…
- 12. PROCEDURE: Done under general anaesthesia Step :1 • If the fetal hand is not prolapsed , bring down a hand …. • A roller gauze is tied on the fetal wrist and an assistant is asked to give traction towards the side away from the fetal head to make the neck more accessible and fixed. Step : 2 two fingers of the left hand are introduced with the palmer surface downwards and the finger tips are to be placed on the superior surface of the neck the proposed site of decapitation. Step :3 The decapitation hook with knife is to be introduced flushed under the guidance of the fingers placed into the vagina the knob pointing towards the fetal head The hook is pushed above the neck and rotated to 90 degree so as to place the knife firmly against the neck
- 13. STEP 4: • By upward and downward movements of the hook with knife the vertebral column is served evident by sudden loss of resistance the rest of the soft tissue left behind may be severed by the same instrument or by embryotomy scissors… • While removing the decapitation hook it is to be pushed up rotated to 90 degree and then to take out under the guidance of the internal fingers…. • The decapitated head is pushed up and the trunk is delivered by traction on the prolapsed arm… Step 5: • delivery of the decapitated head any of the following methods may be usually effective… • By hooking the index finger into the mouth…. • By holding the severed neck with giant valselum and delivery of the head as that of after coming head in breech….. • Using forceps…..
- 14. STEP6: Routine exploration of the utero vaginal canal to exclude rupture of the uterus or any other injury.
- 15. THE BLOND HEIDLER THIMBLE AND DECAPITATING WIRE
- 16. Method of passing the decapitating wire round the fetal neck by means of the blond heidler thimble
- 17. EVISCERATION: • The operation consists of removal of thoracic and abdominal contents piecemeal through an opening on the thoracic or abdominal cavity at the most accessible site. • The objectives is to diminish the bulk of the fetus which facilitates its extraction • It difficulty arises the spine may have to be divided spondylotomy with embryotomy scissors INDICATION : Neglected shoulder presentation with dead fetus the neck is not easily accessible Fetal malformation such as fetal ascites or hugely distended bladder or monsters Thoracic or abdominal tumours….
- 18. • The operation is performed by first making a large opening with a perforator or embryotomy scissors into the abdomen or thorax….. • The viscera are the broken up and removed manually….. • If the thorax has to be incised first the abdominal viscera are reached via the diaphragm…. • During these manipulation if the lie is transverse the trunk of the child may be steadied by pulling down an arm…. • But if that is not possible truck presentation valsella may be employed for this purpose….
- 19. CLEIDOTOMY: • the operation of reduction in the bulk of the shoulder girdle by division of one or both the clavicle to reduce the biacromial diameter ….. • The operation is done only in dead fetus with shoulder dystocia …. • The clavicles are divided by the embryotomy scissors or long straight scissors introduced under the guidance of left two fingers placed inside the vagina … • Indication: • To reduce the width of the shoulder in large fetus that cannot be delivered vaginally… • When maneuvers for shoulder dystocia are unsuccessful..
- 20. • Follow all general principle of conducting destructive operations • Make a small cut in the skin of neck of the fetus • Place one hand vaginally along with the ventral aspect of the fetus and identify clavicle • Use embryotomy scissors and cut the clavicle into two and reduce the width of the shoulder and shoulder and deliver the fetus SPONDYLECTOMY: • Spondylectomy is transection of the spine of the delivered thorax… • In breech presentation it may allow drainage of CSF…. • It is done when the back is anterior and head and the neck are out of reach…. • In cases of hydrocephalus when there is communication between the ventricle and spinal cord the fluid may be drained from brain in this way thus obviating the need for craniotomy…