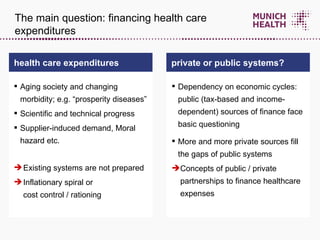
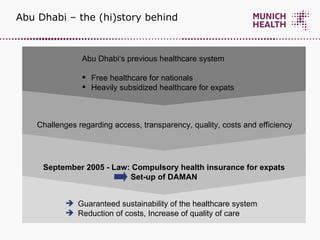
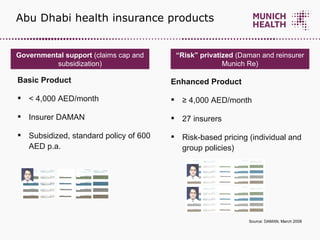
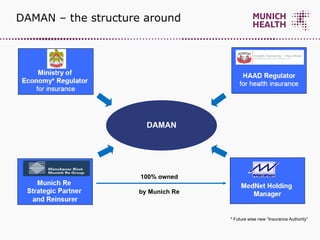
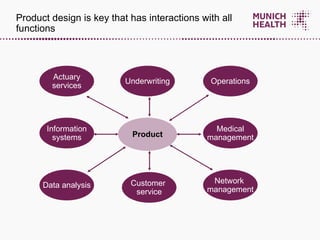
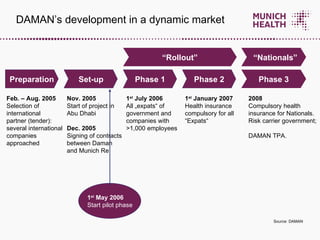
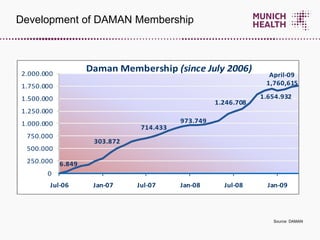
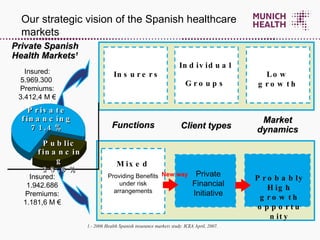
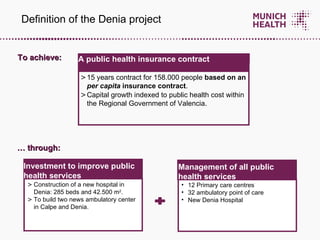
The document discusses public-private partnerships (PPPs) in healthcare systems and provides examples from Abu Dhabi and Denia, Spain. It describes DAMAN, Abu Dhabi's compulsory public health insurance program established through a PPP with Munich Re. It outlines DAMAN's structure, products, and growth over time. It also summarizes the Denia project, a 15-year PPP contract in Spain integrating public health services and facilities under private management. The document concludes that strong private partners with expertise are key to PPP success and that gradual introduction of competition improves access, quality and efficiency.