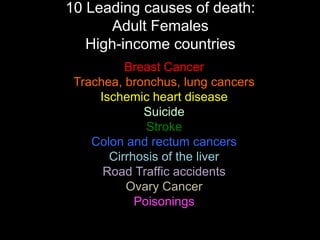
Women face specific challenges related to non-communicable diseases (NCDs) such as cardiovascular disease, chronic respiratory disease, and cancer. The top 10 causes of death for women in both high and low-income countries include several NCDs. Women are more susceptible to NCDs due to biological and societal factors that make prevention and treatment more difficult. Addressing NCDs will be a priority for improving women's health and development globally.