Downloaded 21 times
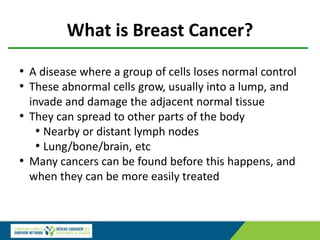








![Mammographic breast density is associated with the
development of contralateral breast cancer
Raghavendra A et al. Cancer 2017; 123:1935-1940
• 229 stage I - III BC between Jan 1997 and Dec 2012
• 451 matched controls
• After adjustment for potential prognostic risk factors for
BC, the odds of developing CBC were found to be
significantly higher for patients with dense breasts (odds
ratio, 1.80; 95% confidence interval, 1.22-2.64 [P<.01])
than for those with non-dense breasts.](https://image.slidesharecdn.com/webinarbreastscreeningandbreastdensity-200214180026/85/WEBINAR-Breast-Screening-and-Breast-Density-94-320.jpg)

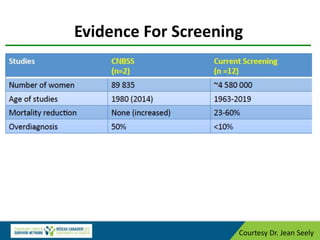
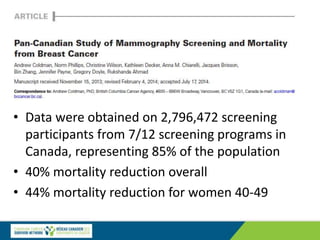
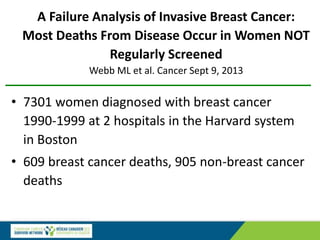
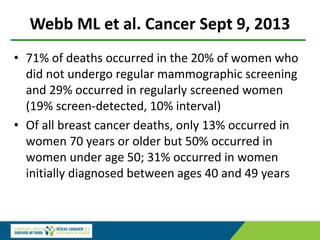
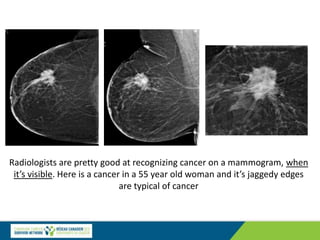
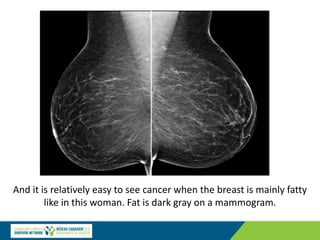
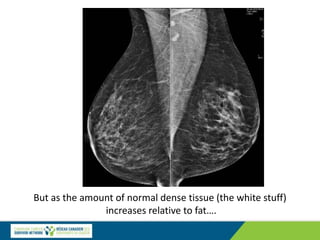
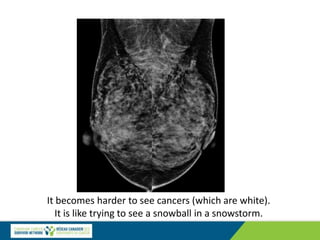
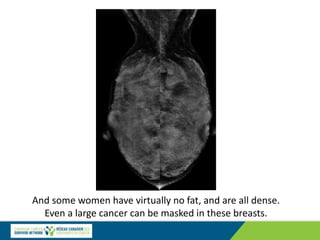
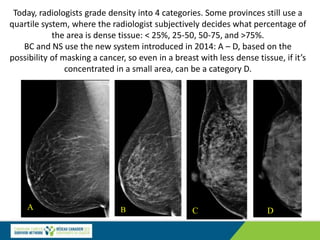
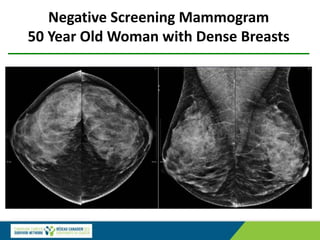
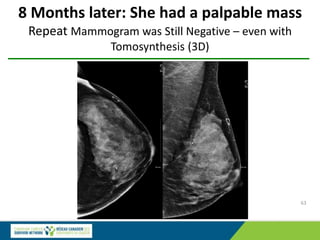
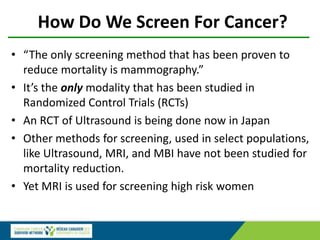
The document discusses the significance of optimal breast cancer screening, emphasizing the need for early detection to enable less aggressive treatments and improve survival rates. It outlines the best practices for screening, the impact of breast density on the detection of cancer, and the conflicting guidelines regarding the age to begin screening. Emphasis is placed on the benefits of annual screenings starting at age 40, particularly for women with dense breast tissue, as well as the risks of overdiagnosis and the importance of making informed choices regarding breast cancer screening.























































































