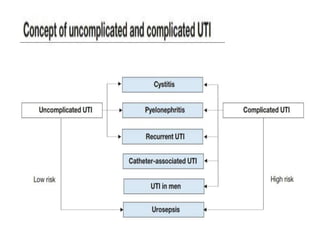
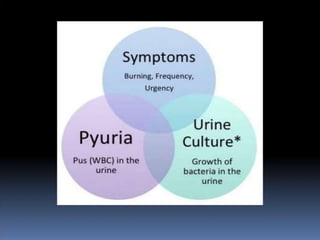
The document discusses urinary tract infections (UTIs). It defines different types of UTIs including asymptomatic bacteriuria, cystitis, prostatitis, and pyelonephritis. Escherichia coli is the most common bacteria responsible. Diagnosis requires a urine culture showing over 105 colony-forming units per mL or symptoms present with a lower count. Treatment duration depends on the infection location, with tissue infections requiring longer therapy. Risk factors include anatomical abnormalities, foreign bodies, and loss of host defenses.



































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














