DEFINITION
Condition in whichmicroorganisms actively multiply
and persist in the genitourinary tract.
Acute infection of the urinary tract falls into two general
anatomic categories.
Lower urinary Tract Infection - Urethritis And Cystitis.
Upper urinary Tract Infection - Acute Pyelonephritis.
4.
OVERVIEW OF UTI
Mostcommon infectious disease.
Affects allages.
Affect women more than men.
5.
WHO ARE ATRISK FOR UTI
More common in adults than in children. Infections
in children are more likely to be serious than those
in adults and should not be ignored.
Pregnancy.
Diabetic /Immunosuppressed individuals
Calculi.
Men with an enlarged prostate.
6.
WHO ARE ATRISK FOR UTI
Any medical conditions that cause incomplete
bladder emptying (spinal cord injury) or bladder
decompensation after menopause.
Catheter associated UTIs
Unsterile procedure while insertion
Prolonged Catheterization
Severe underlying Diseases
Lack of catheter care
7.
CAUSATIVE AGENTS
Mainly causedby colonic bacteria
E.coli – most common
Klebsiella
Proteus
Staphyloccus saprophyticus
Pseudomonas aeruginosa
Candida- infections in Diabetic or imunocompromised
patients.
8.
The most commoncause of UTIs are bacteria from
the bowel that live on the skin near the rectum or
in the vagina, which can spread and enter the
urinary tract through the urethra.
9.
COMMON PRESENTING
SYMPTOMS
Frequent urination,but very little urine may come
out.
Painful burning(dysuria) sensation before, during,
and after urinating.
Urinating blood.
Urgent need to urinate, and in serious cases,
unable to control bladder and leaks urine.
Cloudy or foul smelling urine.
Fever.
Malaise or the general feeling of unwell.
Severe pain in the lower abdominal
region(suprapubic pain).
10.
Cystitis
Involves bladder .
Characterizedby:
Dysuria . Urgency.
Frequency. Suprapubic Pain.
Incontinence . Malodorous Urine.
No fever and does not result in renal injury
CLINICAL MANIFESTATIONS
11.
Urethritis
Suspected in growth/culture negative symptomatic cases
Symptoms similar to Cystitis.
Caused by Sexually Transmitted infections .
12.
Acute Pyelonephritis
Involvement ofrenal parenchyma.
Characterized by:
Early Onset Fever,chills
Abdominal Pain or Flank Pain.
Malaise.
Nausea and Vomiting.
13.
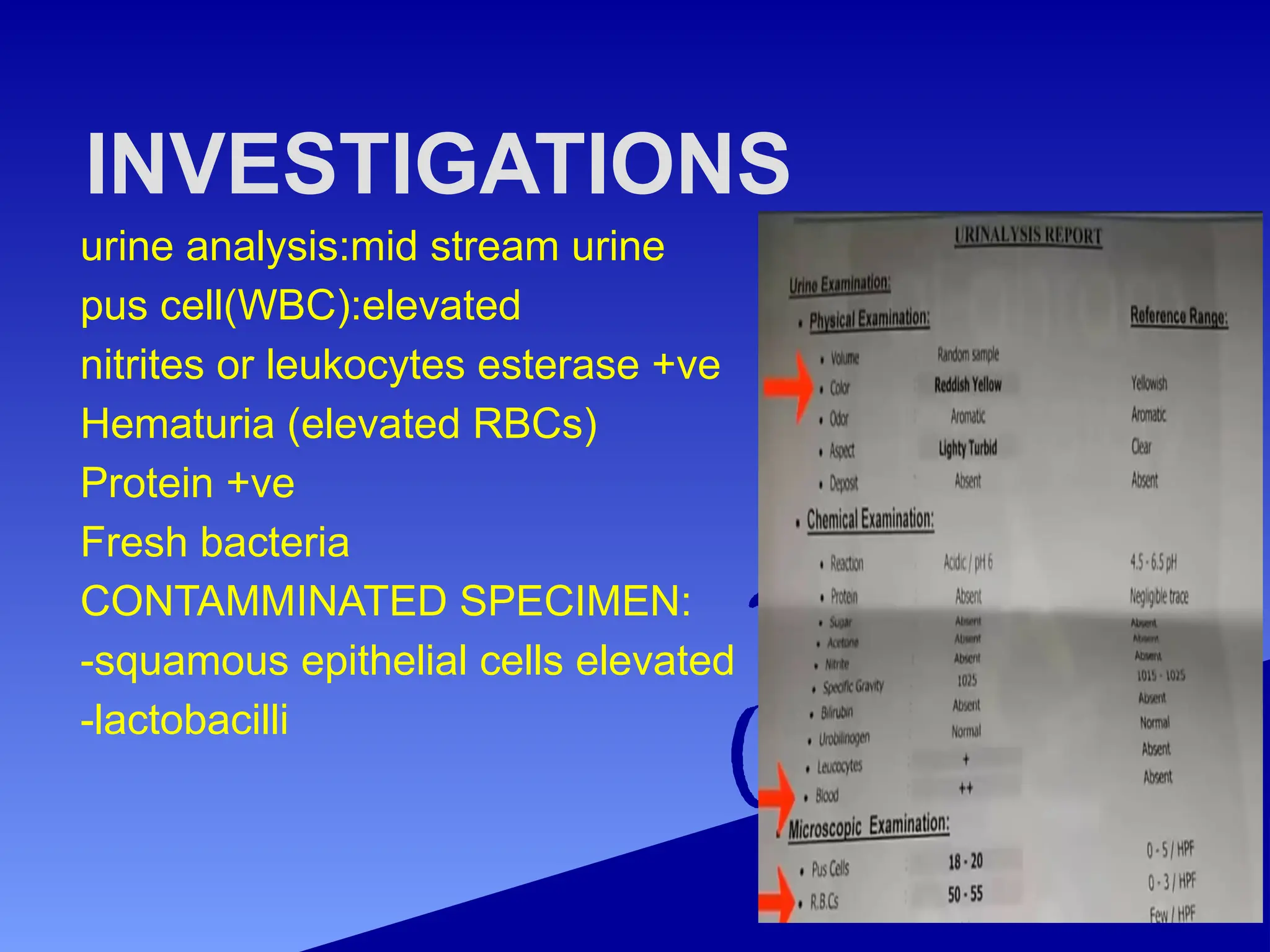
INVESTIGATIONS
urine analysis:mid streamurine
pus cell(WBC):elevated
nitrites or leukocytes esterase +ve
Hematuria (elevated RBCs)
Protein +ve
Fresh bacteria
CONTAMMINATED SPECIMEN:
-squamous epithelial cells elevated
-lactobacilli
COLLECTING URINE FOR
EXAMINATION
SpecimenCollection
The urine collected in a wide
mouthed sterile container
A mid stream specimen is
the most ideal for processing.
Do not collect spontaneously
collected urine , which can
Lead to contamination with
commensal bacterial colonies
on urethral orifice and
perineum.
16.
TRANSPORT OF URINE
Allcollected specimens of
urine to be transported
to laboratory with out delay
Delay of 1-2 hour lowers the
quality of diagnostic
evaluations.
If the delay is anticipated the
specimens are to be preserved
at 40
c.
UPPER URINARY TRACT
INFECTION(PYELONEPHRITIS):-
•INVESTIGATION:
• URINE ANALYSIS:-
• PUS CELLs(WBCs):elevated.
• Nitrrites:may be +Ve.
• leukocyte esterase:may be +Ve
• RBCs:may be elevated.
• Protein:may be +Ve
URINE CULTURE
CBC(LEUKOCYTOSIS)
20.
radiologycal imaging:
• CT-KUB/ CT SCAN(contrast -enhanced
CT of the abdomin and pelvis.
• indication for CT : -
• no improvement after 48-72hours of
antibiotics.
• poorly controlled DM or
immunocompromised patients.
• suspected complication
obstruction,abscess .
TREATMENT
Conservative:
Increased oral fluidsintake.
Acidification of urine.
Regular and complete bladder emptying.
Good personal hygiene.
1st line:-
ciprofloxacin 500mg bid for (7 days).
levofloxacin 750 mg od for (5 days).
2nd line:-
Ampicillin-sulbactam 1.5 g IV/6h (10-14 days).
Ceftriaxone 1g IV /24H(10-14 days).
23.
Asymptomatic bacteriuria
+ urineculture without any
manifestation of infection.
Occurs exclusively in girls, elderly men
and women.
Benign and does not cause renal injury.
24.
ASYMPTOMATIC BACTERIURIA
• TT:-
•AMOXICILLIN-CLAVULUANIC ACID 625
mg every 8H.
• OR
• CEPHALEXIN 500mg EVERY 6 h (7
days).
• recurrent lower UTI:-
• PROPHYLACTIC DAILY ANTIBIOTIC AS
cephalexin 500mg at night.
25.
COMPLICATION:-
• chronic pyelonephritis:-
•recurrent infection cause inflammation and
scarring lead to decrease kidney function
that can end with chronic kidney disease.
• prerenal abscess






















































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)




